

INTRODUCTION
Coronavirus Disease 2019 (COVID-19) is an infectious disease caused by SARS-CoV-2 coronavirus that spread rapidly throughout the world, affecting up to 779 million people and resulting in >7.1 million deaths worldwide1. Physiological and environmental factors were shown to have a significant effect on both susceptibility and severity of COVID-19. Specifically, sex (male), age (>65 years), smoking, as well as various co-morbidities including diabetes, obesity, cardiovascular and respiratory diseases were considered as risk factors for severe COVID-19 and adverse outcome2. In addition, socioeconomic3, meteorological4, and other environmental factors were also shown to affect COVID-19 epidemiology. An association between environmental pollution levels and COVID-19 epidemics was also noted5.
Metals are considered as environmental pollutants, being a component of particular matter6. Toxic metals and metalloids, including arsenic (As), cadmium (Cd), mercury (Hg), and lead (Pb), possess significant health hazards through induction of oxidative stress, endoplasmic reticulum stress, inflammation, and apoptosis, to name a few7. Certain studies have demonstrated that toxic metal(loid) exposure may play a significant role in respiratory diseases8. In this regard, we aimed to assess if toxic metal and metalloid exposure may have contributed to susceptibility and aggravation of COVID-19 through induction of respiratory toxicity, oxidative stress, local and systemic inflammation, and immune dysfunction9. However, the existing data are highly insufficient and lack comparisons with a healthy population10,11.
Therefore, the objective of the present study was to evaluate serum toxic metal(loid) levels in COVID-19 patients of different disease severity, as well as to assess the relationship between serum metal concentrations and key markers of disease severity.
METHODS
Study design and participants
A total of 179 subjects, including 46 healthy controls and 133 COVID-19 patients who were admitted to the inpatient departments for COVID-19 treatment at the Sechenov University Clinical Center, were enrolled in this case-control study. COVID-19 was verified by RT-PCR testing for SARS-CoV-2 for the inclusion of cases. According to computer tomography (CT), COVID-19 cases were classified into stages of lung damage12: CT-1: <25% (mild) (n=55); CT-2: 25–50% (moderate) (n=44); CT-3: 50–75% (severe) (n=34); while CT-4: >75% (critical) cases were not enrolled in the study. Our controls included SARS-CoV-2-negative healthy volunteers who underwent routine examination at the Clinical center who were recruited at a voluntary basis, with no matching performed. All procedures were performed in agreement with the ethical principles of the Declaration of Helsinki (1964) and its later amendments. The protocol of the present study was approved by the Sechenov University Ethics Committee (Moscow, Russia), No. 07-17/13.09.17.
Physical examination
Data on sex and age, body weight and height were registered for subsequent assessment of body mass index (BMI) values. Along with the registration of anthropometric parameters, physical examination also included respiratory rate (RR) and heart rate (HR) per minute. Body temperature was evaluated daily with the use of maximal values (T °C) for statistical analysis. Blood oxygen saturation (SatO2) was evaluated using a pulse oximeter.
Blood serum sampling
Venous blood samples were collected from the cubital vein using ‘Vacuette’ tubes (Greiner Bio-One International AG, 4550 Kremsmünster, Austria) with subsequent centrifugation at 1600g for 10 min for separation of blood serum. The serum was collected into Eppendorf tubes and stored at -40°C until analysis.
C-reactive protein level assessment
Circulating C-reactive protein level being a marker of systemic inflammation was assessed using the respective Randox kit (Randox Laboratories Ltd., Crumlin, UK) with an automated biochemical analyzer.
Toxic metal analysis
Prior to analysis serum samples were subjected to dilution 1:15 (v/v) with an acidified diluent (pH=2.0) consisting of 1-Butanol 1% (Merck KGaA, Germany), Triton X-100 0.1% (Sigma-Aldrich, USA), and HNO3 0.07 % (Sigma-Aldrich, USA) in 18.2 MΩ·cm distilled deionized water (Labconco, USA).
Assessment of serum arsenic (As), cadmium (Cd), mercury (Hg), and lead (Pb) was performed using inductively-coupled plasma mass-spectrometry (ICP-MS) at NexION 300D (PerkinElmer, USA) equipped ESI SC-2 DX4 autosampler (Elemental Scientific, USA). Universal Data Acquisition Standards Kit (PerkinElmer Inc., Shelton, CT, USA) were used for system calibration with the final concentrations of the metal(loids) of 0.5, 5, 10 and 50 μg/L. Internal online standardization was performed using Yttrium (Y) and Rhodium (Rh) Pure Single-Element Standards (PerkinElmer Inc., Shelton, CT, USA). The obtained data on serum metal(loid) levels were expressed as ng/mL. Values lower than limit of detection (LoD) were provided as LoD/2. The certified reference materials of human plasma (ClinChek® Plasma Control, Levels I, II, Lot 1286) were used for laboratory quality control with the recovery rates of 85–117% for all metals assessed.
Statistical analysis
Statistical analysis was performed with Statistica 10 (Statsoft, USA). The obtained data on anthropometric and clinical variables were expressed as mean and standard deviation (Mean ± SD). In turn, serum metal(loid) levels in the studied subjects were expressed as median and interquartile range (IQR) due to a skewed distribution. Moreover, for further processing, the raw values on toxic metal levels were log-transformed using a natural logarithm (Ln) to obtain a log-normal distribution. Due to the role of being overweight/obese13 and having advanced age14 as risk factors for COVID-19 severity, as well as significant variability in demographic and anthropometric parameters between the groups, group comparisons were performed using analysis of covariance (ANCOVA) with adjustment for age, sex, and BMI using Bonferroni adjustment. Analysis of correlation between toxic metal(loid) levels and COVID-19 severity markers was performed using Spearman’s rank coefficient. Furthermore, multiple linear regression analysis was performed in order to estimate independent associations between Ln-transformed toxic metal(loid) levels with percentage of lung damage, SatO2, or CRP as markers of disease severity, after adjustment for demographic and clinical parameters like sex, age, BMI, HR, RR, fever (max T °C) values. Markers of diseases severity like lung damage, SatO2, or CRP were also included as predictors, if not used as a dependent variable. Model 1 included only the above-mentioned demographic and clinical parameters as predictors, whereas Model 2 also included Ln-transformed levels of As, Hg, and Pb as independent predictors. The level of significance was set at p<0.05 for all statistical analyses.
RESULTS
Descriptive characteristics of the study population are noted in Table 1. Consistent with CT grading, lung damage percentage in the CT-2 (moderate) and CT-3 (severe) groups significantly exceeded that in CT-1 (mild) group by a factor of nearly 2 and 3, respectively (Table 2).
Table 1
Demographic and anthropometric parameters of the studied groups (N=179)
| Parameter | Control (N=46) Mean ± SD | Cases with CT-1 (N=55) Mean ± SD | Cases with CT-2 (N=44) Mean ± SD | Cases with CT-3 (N=34) Mean ± SD |
|---|---|---|---|---|
| Age (years) | 55.48 ± 4.37 | 52 ± 15.51 | 55.36 ± 16.62 | 62.91 ± 14.32a |
| Height (cm) | 172 ± 7.9 | 170.9 ± 9.7 | 169.3 ± 10.8 | 169.5 ± 10.4 |
| Weight (kg) | 78.8 ± 9.59 | 87.57 ± 21.65a | 92.48 ± 22.08a | 88.87 ± 16.57a |
| BMI (kg/m2) | 26.6 ± 2.48 | 30.09 ± 8.1a | 32.08 ± 6.22a | 30.41 ± 5.53a |
Table 2
Clinical and laboratory markers of COVID-19 severity in controls and cases with various CT grades (N=179)
| Parameter | Control (N=46) Mean ± SD | CT-1 (N=55) Mean ± SD | CT-2 (N=44) Mean ± SD | CT-3 (N=34) Mean ± SD | p trend |
|---|---|---|---|---|---|
| HR (bpm) | 73.87 ± 6.41 | 82.56 ± 13.9a | 84.93 ± 11.45a | 88.24 ± 14.03a | <0.001 |
| RR (rpm) | 17.98 ± 1.56 | 19.73 ± 2.2a | 20.26 ± 2.37a | 21.6 ± 4.4a,b | <0.001 |
| Fever (max T °C) | 36.6 ± 0.09 | 38.21 ± 0.69a | 38.2 ± 0.67a | 38.18 ± 0.72a | <0.001 |
| SatO2 (%) | 97.91 ± 0.81 | 95.15 ± 3.17a | 93.45 ± 5.9a | 88.03 ± 7.76a,b,c | <0.001 |
| CRP (mg/L) | 1.92 ± 1.4 | 53.97 ± 70.39a | 86.77 ± 83.99a,b | 143.25 ± 88.54a,b,c | <0.001 |
| Lung damage (%) | 0 | 22.45 ± 5.84 | 44.27 ± 11.17b | 61.71 ± 11.21b,c | <0.001 |
a,b,c Significant group difference as compared to the control, CT-1, and CT-2 group values at p<0.05, respectively. CT: computer tomography grade of lung damage: CT-1: <25% (mild). CT-2: 25–50% (moderate). CT-3: 50–75% (severe). HR: heart rate, beats per minute. RR: respiratory rate, respirations per minute. SatO2: blood oxygen saturation. CRP: C-reactive protein.
COVID-19 patients were characterized by significantly higher heart rate, exceeding the control values in subjects with mild, moderate, and severe lung damage by 12% (p=0.029), 15% (p<0.001), and 19% (p<0.001), respectively. Although the severity-related trend to an increase in HR was significant, no substantial group difference in COVID-19 patients was observed. COVID-19 was also shown to be associated with dyspnea. Specifically, respiratory rate in subjects with mild, moderate, and severe lung damage exceeded the respective control values by 10% (p=0.051), 13% (p<0.001), and 20% (p<0.001). Moreover, patients with severe lung damage (CT-3) were characterized by 9% (p=0.012) higher RR compared to subjects with mild lung damage (CT-1). The overall trend for severity-associated increase in RR was also highly significant (p<0.001).
Patients with COVID-19 were also characterized by fever, exceeding the body temperature of the healthy controls by 4% (p<0.001). However, no significant difference was observed between groups of patients with varying degrees of lung damage severity.
Of all studied markers of the disease severity, the circulating CRP level was characterized by the most profound group difference. Specifically, CRP concentration in COVID-19 patients with mild, moderate, and severe lung damage significantly exceeded the control values by a factor of more than 28 (p=0.008), 45 (p<0.001), and 74 (p<0.001), respectively. Moreover, CRP levels in patients with the highest disease severity were significantly higher than those of patients with CT-1 and CT-2 degrees by 265% (p<0.001) and 65% (p=0.001), respectively. Blood oxygen saturation (SatO2) was characterized by a severity-associated decline. Specifically, SatO2 values in COVID-19 patients with mild (CT-1), moderate (CT-2), and severe (CT-3) lung damage were 3% (p=0.008), 5% (p<0.001), and 10% (p<0.001) lower than the control values, respectively. Moreover, in the most severe COVID-19 cases, SatO2 was characterized by a significant decrease by 7% (p<0.001) and 2% (p<0.001) when compared to the respective CT-1 and CT-2 group values.
In parallel with markers of lung damage and inflammation, serum toxic metal(loid) levels were also significantly associated with COVID-19-associated lung damage (Figure 1). Specifically, serum As concentrations in COVID-19 patients with mild (CT-1), moderate (CT-2), and severe (CT-3) lung damage were approximately 3-fold higher than the respective control values. No significant group difference between the groups of patients with different COVID-19 severity grading was observed.
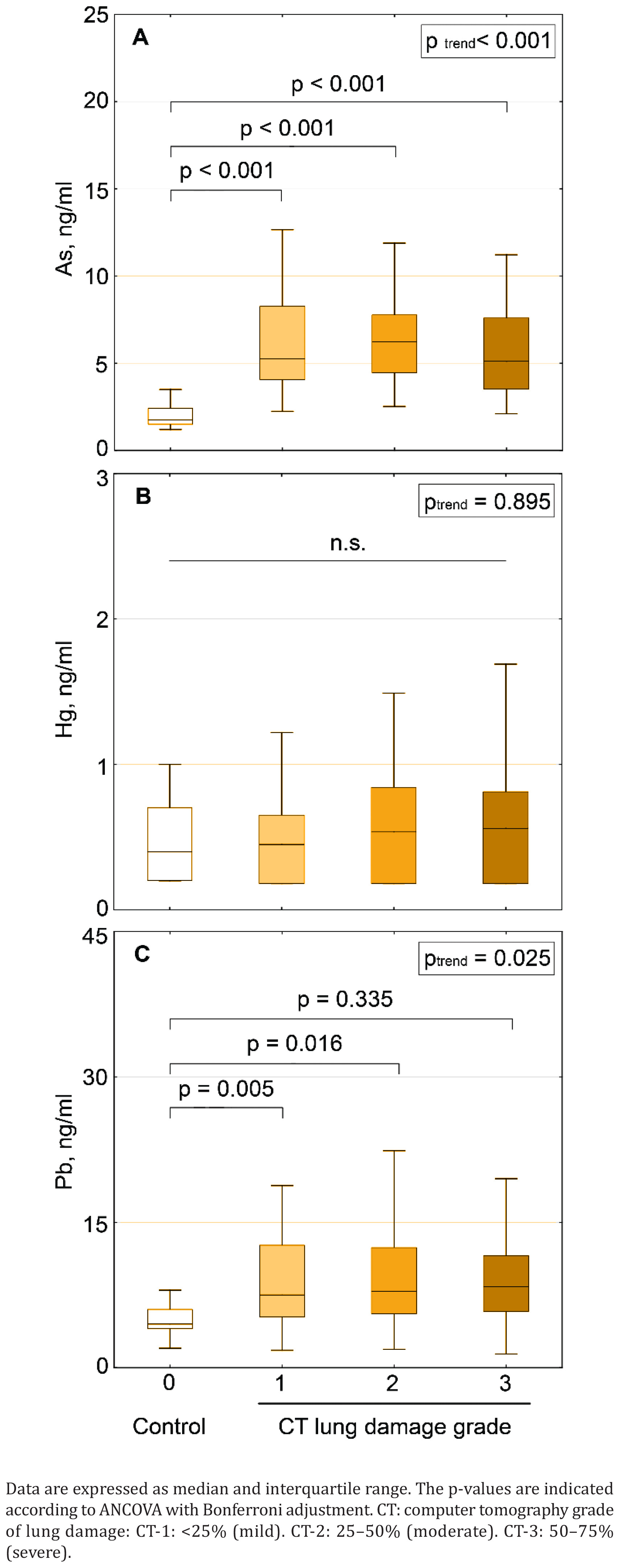
Serum Pb levels were also characterized by a COVID-19-associated increase. Circulating Pb concentrations in patients with mild (CT-1) and moderate (CT-2) lung damage exceeded that in healthy examinees by 67% and 76%, respectively. Despite 87% higher serum Pb concentrations in patients with severe lung damage (CT-3), the difference in comparison to controls was not significant.
Although serum Hg concentrations tended to increase in patients with COVID-19 in a severity-dependent manner, the observed differences were not significant and statistically indistinguishable from controls.
Serum Cd levels were also evaluated, although the majority of subjects from both control and case groups were characterized by concentrations lower than the level of detection. Detectable Cd levels were revealed in the serum of 12%, 15%, 21%, and 23% of subjects from the control, mild (CT-1), moderate (CT-2), and severe (CT-3) groups, respectively.
Correlation analysis (Table 3) demonstrated a significant association between toxic metal(loid) levels and COVID-19 severity markers. Specifically, serum As levels positively correlated with fever, percentage of lung damage, and CRP concentration, being inversely associated with SatO2. Circulating Pb levels were also significantly correlated with fever and lung damage percentage, although the observed associations were weaker compared to those observed for As. Finally, serum Hg levels significantly correlated only with CRP concentration at the border of significance.
Table 3
Correlation analysis between serum As, Pb, and Hg levels and the COVID-19 severity markers
| Parameter | Ln (As) | Ln (Pb) | Ln (Hg) | |||
|---|---|---|---|---|---|---|
| r | p* | r | p* | r | p* | |
| SatO2 (%) | -0.175 | 0.019 | -0.102 | 0.174 | 0.028 | 0.713 |
| Fever (max T °C) | 0.480 | <0.001 | 0.263 | <0.001 | 0.061 | 0.416 |
| Lung damage (%) | 0.455 | <0.001 | 0.297 | <0.001 | 0.125 | 0.095 |
| CRP (mg/L) | 0.227 | 0.002 | 0.123 | 0.102 | 0.149 | 0.046 |
In view of significant group difference in toxic metal(loid) concentration and its correlation with COVID-19 severity markers, multiple linear regression analysis was performed in order to evaluate independent associations between toxic metal levels and lung damage, CRP, and SatO2 after adjustment for other anthropometric and clinically important variables (Table 4).
Table 4
Multiple regression analysis of the association between lung damage (%), CRP, and SatO2 (dependent variables) and serum toxic metal levels
| Predictor | Lung damage | CRP | SatO2 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 1 | Model 2 | Model 1 | Model 2 | |||||||
| β | p* | β | p* | β | p* | β | p* | β | p* | β | p* | |
| Lung damage | - | - | - | - | 0.200 | 0.006 | 0.207 | 0.007 | -0.173 | 0.022 | -0.193 | 0.015 |
| CRP | 0.220 | 0.006 | 0.209 | 0.007 | - | - | - | - | -0.446 | <0.001 | -0.453 | <0.001 |
| SatO2 | -0.175 | 0.022 | -0.179 | 0.015 | -0.412 | <0.001 | -0.417 | <0.001 | - | - | - | |
| Sex | -0.076 | 0.187 | -0.048 | 0.387 | 0.082 | 0.135 | 0.071 | 0.199 | 0.032 | 0.572 | 0.031 | 0.594 |
| Age | 0.015 | 0.812 | 0.016 | 0.790 | 0.069 | 0.234 | 0.072 | 0.220 | -0.224 | <0.001 | -0.213 | <0.001 |
| BMI | 0.092 | 0.122 | 0.059 | 0.307 | 0.201 | <0.001 | 0.192 | 0.001 | 0.122 | 0.038 | 0.108 | 0.070 |
| HR | 0.094 | 0.160 | 0.086 | 0.183 | 0.079 | 0.216 | 0.081 | 0.204 | 0.006 | 0.928 | 0.011 | 0.872 |
| RR | 0.107 | 0.103 | 0.127 | 0.051 | 0.080 | 0.202 | 0.065 | 0.321 | -0.073 | 0.262 | -0.078 | 0.250 |
| Fever | 0.281 | <0.001 | 0.165 | 0.016 | 0.077 | 0.233 | 0.095 | 0.164 | -0.079 | 0.239 | -0.087 | 0.220 |
| Ln (As) | - | - | 0.223 | 0.001 | - | - | -0.036 | 0.580 | - | - | 0.031 | 0.651 |
| Ln (Pb) | - | - | 0.083 | 0.149 | - | - | -0.032 | 0.571 | - | - | 0.013 | 0.832 |
| Ln (Hg) | - | - | 0.035 | 0.523 | - | - | 0.093 | 0.085 | - | - | 0.098 | 0.080 |
| Multiple R | 0.703 | 0.739 | 0.735 | 0.742 | 0.708 | 0.715 | ||||||
| Multiple R2 | 0.494 | 0.546 | 0.540 | 0.550 | 0.501 | 0.512 | ||||||
| Adjusted R2 | 0.470 | 0.516 | 0.519 | 0.521 | 0.478 | 0.480 | ||||||
| p of model | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | ||||||
* Association is significant at p<0.05. SatO2: blood oxygen saturation. CRP: C-reactive protein; BMI: body mass index. HR: heart rate. RR: respiratory rate. Ln: natural logarithm-transformed metal level. Model 1: sex, age, BMI, HR, RR, fever (max T °C) are used as independent predictors plus CRP and SatO2 for prediction of lung damage, or lung damage and SatO2 for prediction of CRP, or lung damage and CRP for prediction of SatO2. Model 2: parameters included in Model 1 plus Ln-transformed levels of As, Hg, and Pb as independent predictors.
The crude model based on the clinical and anthropometric variables accounted for 47% of lung damage variability. CRP and fever were considered as significant positive predictors, whereas SatO2 was inversely associated with lung damage percentage. At the same time, including log-transformed values of serum metal levels increased the predictive potential of the model by 5% (to 52%). Moreover, serum As level was found to be positively associated with lung damage even after adjustment for other variables, including CRP, SatO2, and fever.
Circulating CRP levels were found to be significantly positively and negatively associated with lung damage percentage and blood oxygen saturation, respectively. Moreover, higher BMI values also predicted elevated CRP concentrations. The overall model adjusted for clinical and anthropometric variables also possessed significant predictive potential, accounting for up to 52% of CRP variability. At the same time, including log-transformed metal(loid) levels into the model did not affect its predictive ability. Only serum Hg levels tended to be associated with CRP levels, although this association was only nearly significant (p<0.1).
Similar patterns were revealed in the next regression model with SatO2 being the dependent variable. Briefly, in a crude model based on anthropometric and clinical variables, CRP, lung damage, and age were found to be inversely associated with blood oxygen saturation. In turn, BMI values were characterized by a positive association with SatO2 at the border of significance. As in the case of CRP, inclusion of metal levels into the model did not improve its predictive potential.
DISCUSSION
Our study demonstrated an association between elevated As and Pb levels with markers of disease severity in COVID-19 patients. Only serum As concentrations were characterized by a direct independent association with lung damage percentage in adjusted models. These findings corroborate our earlier hypothesis on the potential association between toxic metal(loid) exposure and higher COVID-19 susceptibility and severity9. Other studies also assessed metal levels in COVID-19 patients in relation to the disease severity, with unclear findings. Specifically, Zeng et al.10 demonstrated significantly lower whole blood As and Pb levels in patients with severe illness compared to moderate disease, whereas no association between COVID-19 severity and both Hg and Cd was revealed. Elevated Cd and reduced As levels in whole blood were shown to be related to unfavorable COVID-19 outcomes10. The authors also reported significantly lower urinary Cd, Hg, and Pb levels, as well as elevated As concentrations in patients with severe COVID-19 compared to non-severe forms11. However, no comparison with healthy controls was performed in these studies.
Generally, the noted associations demonstrate that in COVID-19 patients, elevated toxic metal levels are associated with disease severity, in agreement with the earlier data on cytotoxicity of As and Pb for lung cells, as well as their proinflammatory effect. Specifically, the potentiating role of As in the development of viral lung damage is expected to be associated with direct cytotoxicity of As to lung cells15 due to induction of oxidative stress, apoptosis, and genotoxicity16. These findings are in line with the earlier reported association between chronic As exposure and the incidence of non-malignant lung diseases17.
The observed association between serum As levels and CRP is indicative of the potential role of As exposure in development of lung and systemic inflammation. Low-dose As exposure was shown to induce lung inflammation in mice18 that may be mediated by up-regulation of MAPK p38, JNK, ERK1/2, and NF-kB pathways, as well as dysregulation of Th1/Th2 and Th17/Treg differentiation19. RAGE activation may be also considered as the potential mechanism of proinflammatory effect of As exposure in the lungs20. Epidemiological data also demonstrate a significant association between As exposure and lung inflammation21 as well as circulating CRP levels in adults22. Although direct data on the potential impact of As exposure on SARS-CoV-2-induced lung damage are lacking, previous findings demonstrated that As may aggravate virus-induced lung damage. Specifically, As exposure resulted in higher mortality and increased pulmonary virus titers in mice23. Correspondingly, As was shown to aggravate H1N1-induced respiratory dysfunction in adults24.
Serum Pb levels were also characterized by a significant elevation and independent association with COVID-19 severity. Similarly to As, Pb exposure was also shown to induce oxidative stress, mitochondrial dysfunction, as well as cell cycle arrest and apoptosis, altogether resulting in cytotoxicity for human alveolar epithelial cells25. These findings are also supported by the observation of altered respiratory function in Pb-exposed workers even without manifest respiratory disease26. Pb exposure was shown to induce inflammation through up-regulation of proinflammatory cytokine expression and activation of proinflammatory enzymes27 through modulation of NF-κB and AhR signaling28 and promotion of NF-κB translocation29. Correspondingly, Pb exposure induced inflammatory response in vivo30, which was also associated with systemic inflammation in humans22. In parallel with alterations in inflammatory responses, Pb exposure also led to immune dysregulation31, resulting in increased susceptibility to bacterial and viral pathogens32. Finally, a weak correlation was revealed between environmental Pb levels and COVID-19 incidence and mortality in California5, thus addressing the potential role of toxic metal exposure as an independent risk factor of higher COVID-19 susceptibility and severity.
Although no significant elevation in circulating Hg levels was observed in patients with COVID-19, serum Hg concentration was shown to be associated with CRP levels, a marker of systemic inflammation. These findings corroborate a significant direct correlation between serum Hg levels and CRP as a marker of systemic inflammation22. In agreement, earlier studies also demonstrated that Hg may possess toxic effects in the respiratory system. Specifically, methylmercury exposure was shown to induce alveolar cell death through induction of oxidative stress, mitochondrial dysfunction, and apoptosis33, altogether resulting in alteration of lung ultrastructure34. In the present study no significant association between COVID-19 severity and serum Cd levels was observed due to high number of subjects with undetectable serum Cd levels both in cases and controls. However, Cd exposure may be also considered as a potential risk factor of lung damage aggravation due to its cytotoxic and pro-inflammatory effects, as clearly indicated in the case of H1N1 influenza35 and respiratory syncytial36 virus-induced lung damage.
Limitations
The study has several limitations that have to be addressed in further research. First, the case-control design of this study does not provide an insight into the causal relationship between COVID-19 severity and serum metalloid levels. Specifically, lung damage or the severity of COVID-19 could lead to increased absorption of heavy metals rather than the metals causing the lung damage. Therefore, experimental studies aimed at assessing the impact of metal exposure on susceptibility and development of viral infections like COVID-19 may provide insight into the particular role of As and Pb on disease severity. Dose-dependent and time-dependent effects of metal exposure on disease severity also have to be investigated. In addition, other confounding factors like exposure to air pollution, socioeconomic status, and underlying health conditions may also have a significant impact on both serum metal levels and lung damage. Finally, the study is performed in relatively small groups of examinees, with cases not matched with controls, and thus, the obtained data may be extrapolated to other populations with caution.
CONCLUSIONS
The study findings demonstrate that elevated As and Pb levels in COVID-19 patients are associated with disease severity as evidenced by lung damage and systemic inflammatory response. However, the causal relationship between COVID-19 severity and increased body metal burden is yet to be elucidated.