

INTRODUCTION
There is a growing interest in transparency around metals and other impurities in foods, particularly those consumed by children. In 2019, a United States (US) House of Representatives Committee on Oversight Reform began investigating the presence of inorganic arsenic (As), lead (Pb), cadmium (Cd), and mercury (Hg) in baby foods sold in the US and found that these elements were present in products made by all responding companies1. In 2021, the US Food and Drug Administration (FDA) launched the Closer to Zero initiative, which aims to reduce dietary exposures to contaminants to the lowest levels feasible while maintaining access to nutritious foods2-4. As part of this initiative, the FDA prioritized measuring and reducing concentrations of arsenic, lead, cadmium, and mercury in foods commonly consumed by children3,4. Recently enacted and pending regulations in several US states (e.g. California5, Illinois6, New York7) require that baby food manufacturers that sell products in that state test samples monthly for arsenic, lead, cadmium, and mercury, and make the test results publicly available on the company’s website and product labels. Due to the state-specific, patchwork nature of these regulations and the challenges of limiting product sales to within a given state, baby food manufacturers across all US states will likely need to comply with these testing requirements.
Metals and metalloids such as arsenic, lead, cadmium, and mercury (commonly referred to as ‘heavy metals’) occur naturally in the environment and are often detected at measurable concentrations in whole, processed, and packaged foods. At sufficient doses, dietary exposure to heavy metals has been associated with carcinogenic and non-carcinogenic adverse health effects8-12. Monitoring impurities in foods is therefore important for protecting vulnerable populations, particularly children. Under current regulatory requirements, however, consumers are typically provided only with analytical test results indicating the presence and concentration of a given element, without context regarding whether consumption of the product is expected to meaningfully increase health risks. Interpreting these data is further complicated by limited survey information on expected intake of multi-ingredient baby foods, as well as limited evaluation of comparable metal exposures from alternative food options. As state legislation expands public access to testing data, consumers increasingly need guidance on how to interpret reported metal concentrations and whether changes to purchasing decisions are warranted.
The aims of this study were to: 1) use publicly available manufacturer-reported concentrations of arsenic, lead, cadmium, and mercury in baby food products to estimate potential metal exposures for child consumers; and 2) compare these estimated exposures with element-specific regulatory guidelines to evaluate whether consumption of these products may pose a health risk.
METHODS
Overview
In response to new regulations issued in August 2025 requiring baby food manufacturers to monitor and report heavy metals in their products, Consumer Reports – a US-based consumer advocacy organization – reviewed 39 baby food brands and evaluated how easily caregivers could determine heavy metal concentrations in the foods they purchased13. Consumer Reports found that 16 brands earned their highest rating, meaning that the brand made test results for all their products easily accessible on the company’s website.
In September 2025, we reviewed these manufacturers’ websites and found that analytical results could be accessed without a product-specific universal product code (UPC), batch number, or date code for only nine brands. For this subset, we extracted all available analytical results (n=1362 products) and created a database containing brand, product name, and concentrations of arsenic, lead, cadmium, and mercury, reported as parts per billion (ppb) (see Supplementary file). For many products, concentrations were reported as ‘below the limit of detection’ (<LOD). Although the LOD was not always specified, California Assembly Bill (AB) 899 requires that LODs be no greater than 6 ppb (6 μg/kg)14. For each element, at least one product was reported with a detectable concentration below 6 ppb, indicating that analytical methods are capable of detecting and quantifying concentrations below this threshold (Table 1).
Table 1
Summary of arsenic, lead, cadmium, and mercury concentrations (ppb) reported by 9 out of 39 manufacturers of baby food in the US
[i] LOD: limit of detection; differs by food manufacturer and by sample but is required under California AB-899 to be no greater than 6 ppb. For additional details see the Supplementary file. These data may not be representative of the entire baby food market and should be interpreted with caution.
To estimate exposure doses using these reported heavy metal concentrations, we evaluated three scenarios: 1) the element concentration was assumed to be the lowest detected concentration across all products and brands; 2) the element concentration was assumed to be the maximum allowable LOD (i.e. 6 ppb); and 3) the element concentration was assumed to be the highest detected concentration across all products and brands. The maximum allowable LOD assessment (Scenario 2) provides an estimate of the highest possible exposure dose should a manufacturer report the concentration as ‘<LOD’ without also reporting the LOD for their analysis.
Estimates of expected intake for these food types, which include multi-ingredient snacks and meals, were not available, as food intake survey data (e.g. NHANES; US EPA Exposure Factors Handbook) either report single-ingredient intake or multi-ingredient foods that did not align with the foods considered in our analysis. Consequently, we considered a range of possible intake values for each exposure scenario, based on professional judgment and the recognition that some families may rely on these products as a primary food source, while others may have more limited intake.
To evaluate the potential for elevated health risk with consumption of these foods, we compared our exposure dose estimates to available health benchmarks. These element-specific guidance values are expressed as: 1) allowable concentration in food (ppb); 2) permissible daily intake (mg/day); and/or 3) permissible body weight-adjusted dose (mg/kg bw-day).
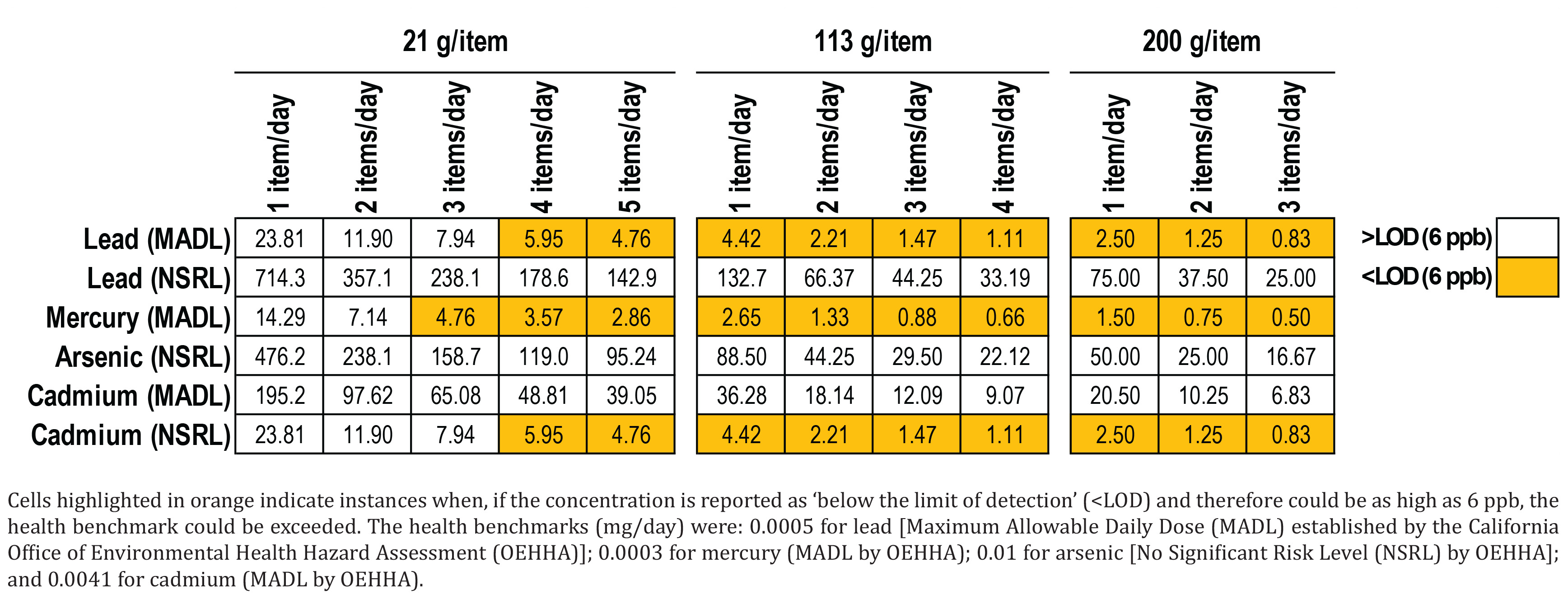
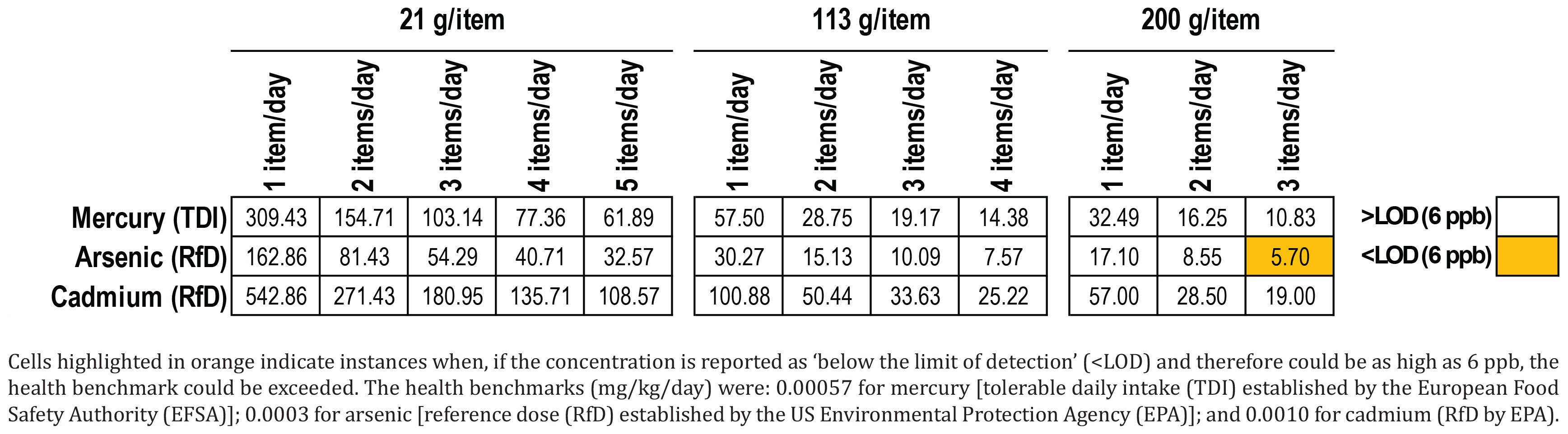
Because reported concentrations are expected to change over time as products continue to be tested, we also estimated the element-specific concentration at which each health benchmark would be reached across a range of intake assumptions. This allows caregivers to review concentration data reported on a manufacturer’s website and, based on the number of products the child will likely consume, quickly determine how the exposure dose will compare to health guidance, which is often reported in units of intake or body weight-adjusted dose.
Allowable concentration
The US FDA has established an action level of 10 ppb for lead in processed foods intended for babies and young children15. At the time of this study, the US FDA had not established an action level for arsenic, cadmium, or mercury. Accordingly, we compared lead concentrations reported by baby food manufacturers directly to this allowable concentration.
Permissible daily intake
Under the California Safe Drinking Water and Toxic Enforcement Act of 1986 (referred to as Proposition 65), the California Office of Environmental Health Hazard Assessment (OEHHA) has established health benchmarks for certain chemicals16. These include the safe harbor levels, namely No Significant Risk Levels (NSRLs) [in μg/day: 10 (arsenic), 15 (lead), 0.05 (cadmium)] for cancer-causing chemicals and Maximum Allowable Dose Levels (MADLs) [in μg/day: 0.5 (lead), 4.1 (cadmium), 0.3 (mercury and mercury compounds)] for chemicals causing reproductive toxicity, and represent maximum acceptable daily intakes. There is no NSRL available for mercury, and no MADL available for arsenic.
To compare manufacturer-reported concentrations to these health benchmarks, we estimated a child’s potential daily baby food intake (kg) based on the mass of the products sold by the nine manufacturers included in our analysis. Products most commonly consisted of pureed food blends sold in ready-to-eat pouches; freeze-dried snacks, puff snacks, and full meals were also included. Portion sizes ranged from 21 to 200 g, with food pouches most often weighing either 99 or 113 g. Accordingly, we selected three representative serving sizes for analysis: 21 g (snack), 113 g (higher reported pouch size), and 200 g (full meal).
Because estimates of typical intake of these mixed-ingredient foods among US children are not available and to accommodate a range of dietary preferences, we assumed that a child may consume up to five snack-size items per day, four pouch-size items per day, or three full meals per day. For each metal, we evaluated three concentration scenarios: the lowest reported concentration, the maximum allowable LOD (i.e. 6 ppb), and the highest reported concentration. These scenarios yield lower-bound and upper-bound exposure estimates, and a worst-case interpretation of exposure if the manufacturer reported only that the concentration was below an unspecified LOD.
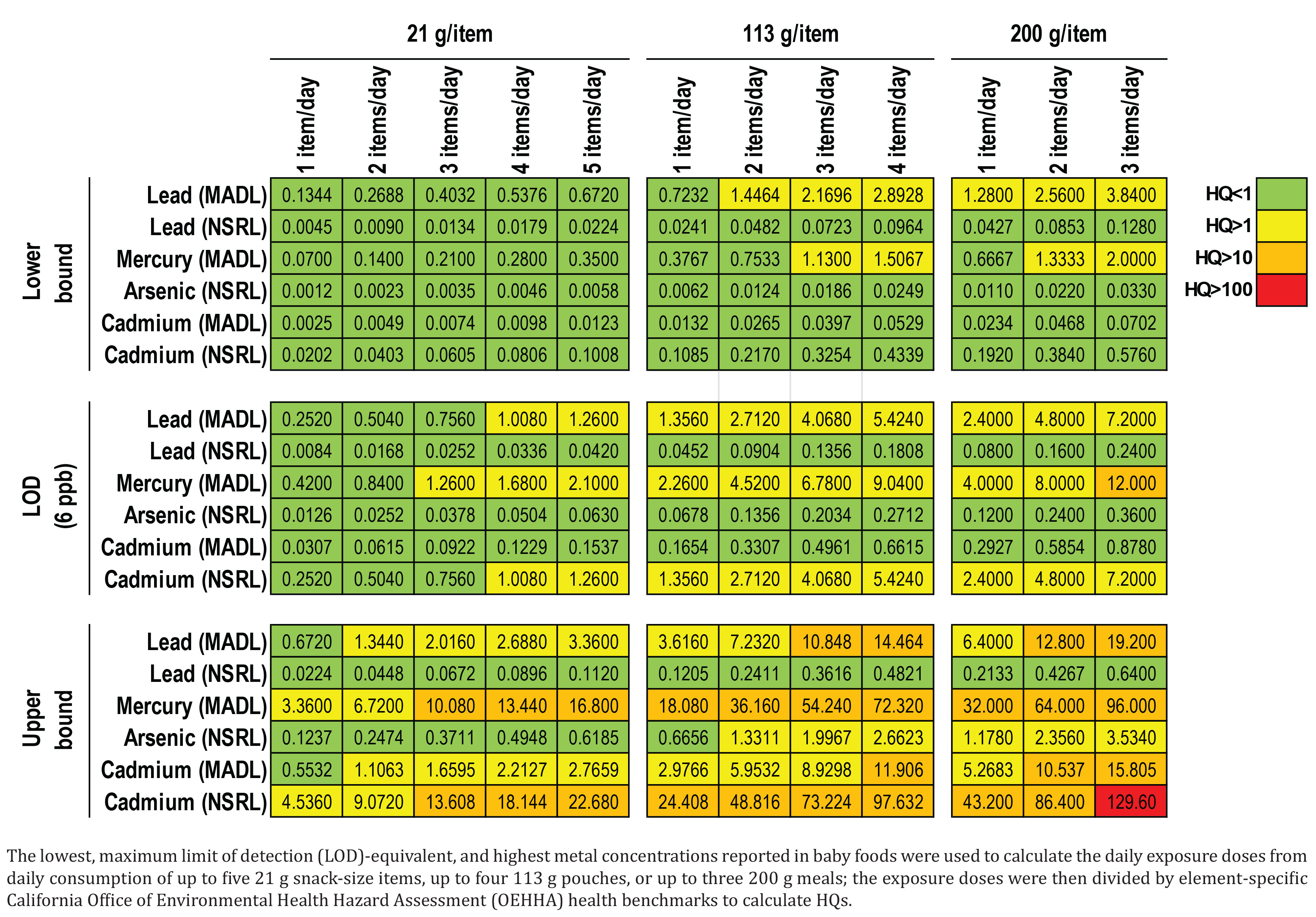
We converted the manufacturers’ reported concentrations (ppb) to mg/kg, converted our estimates of daily intake (g/day) to kg/day, and multiplied these inputs to estimate potential daily exposure (mg/day) to generate an estimate of expected daily intake. We then calculated element-specific hazard quotients (HQs) by dividing the intake estimates by the maximum acceptable daily intake health benchmarks reported by OEHHA. Additional methodological details are provided in the Supplementary file.
It is noteworthy that baby foods are typically consumed for a small fraction of a person’s overall lifetime (approximately 4 out of 70 years). Because NSRLs are designed to be protective against lifetime exposures, it is common to apply a lifetime exposure adjustment to account for the shorter duration exposure. Applying such an adjustment would reduce the HQs estimated in this analysis. Additional methodological details are provided in the Supplementary file.
Permissible body weight-adjusted dose
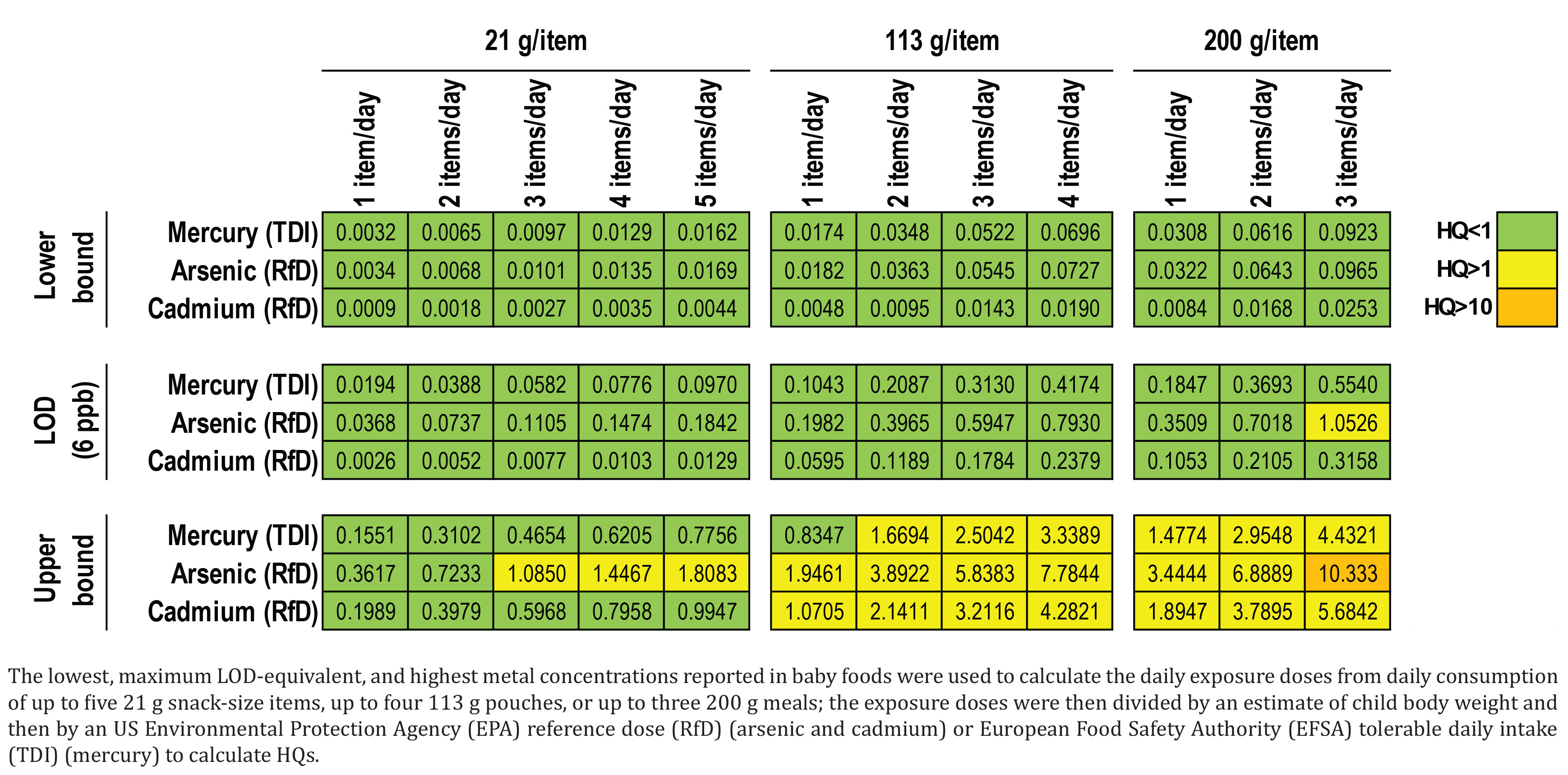
The US Environmental Protection Agency (EPA) has established reference doses (RfDs) for inorganic arsenic (0.3 μg/kg bw-day)17 and cadmium (1.0 μg/kg bw-day)18, whereas the European Food Safety Authority (EFSA) has established a tolerable daily intake (TDI) for inorganic mercury (0.57 μg/kg bw-day)19. No RfD or TDI values are available for lead. To compare estimated exposures to these health benchmarks, we multiplied the manufacturers’ reported element-specific concentrations (mg/kg) by estimates of daily intake (kg/day) and estimates of a typical infant body weight at ages 1 to less than 2 years (11.4 kg) extracted from the EPA Exposure Factors Handbook20. All other assumptions were the same as those used in comparisons to OEHHA benchmarks. Additional methodological details are provided in the Supplementary file.
RESULTS
Allowable concentration
Reported lead concentrations ranged from <LOD to 16 ppb, with the lowest reported concentration of 3.2 ppb (Table 1), indicating that in some products, the action level was exceeded. Because market share data for these products are not available, it is unclear whether these results reflect the full range of lead concentrations in products available for purchase or the likelihood that consumers would purchase a product with lead concentration above or below the action level.
Permissible daily intake
Benchmark exceedances were observed for lead and mercury under lower-bound concentration scenarios when the consumed item was a pouch or a full meal, whereas no exceedances were observed for a snack-size item, even when five items were consumed per day (Figure 1). Under the maximum LOD-equivalent metal concentration scenarios, benchmark exceedances were observed for lead, mercury, and cadmium, with no exceedances for arsenic. Under upper-bound concentration scenarios, benchmark exceedances were identified for all exposure permutations except arsenic when consumed in a snack product.
Permissible body weight-adjusted dose
No benchmark exceedances were observed for mercury, arsenic, or cadmium under lower-bound reported concentrations for all items and intake assumptions (Figure 2). Under the maximum LOD-equivalent concentrations, health benchmark exceedances were noted only for arsenic with the consumption of three meal products per day. Under upper-bound concentration scenarios, benchmark exceedances occurred for mercury, arsenic, and cadmium when the consumed item was a pouch or a meal, whereas for a snack-size item, exceedances were noted for arsenic only.
Metal concentrations in baby food required to reach health benchmarks
The acceptable metal concentration in a food product will vary depending on the health benchmark and the number and size of the food items that will be consumed in a day (Figures 3 and 4). It is also important to consider additional dietary exposures to these metals from other foods consumed. These calculations emphasized that, particularly for lead, mercury, and cadmium, for products where the concentration is reported as below the LOD (without further clarification as to whether this LOD is lower than 6 ppb), consumption could still result in an estimated exposure that exceeds the OEHHA health benchmarks. Additional details on the health benchmarks are provided in the Supplementary file.
DISCUSSION
This analysis demonstrates that reporting heavy metal concentrations alone (i.e. hazard) is insufficient to support informed, risk-based decision-making, particularly for caregivers who may lack the training needed to interpret these data. We provide a health risk interpretation of the available data and also offer a guidance tool that caregivers can use to determine health risk based on reported concentrations and a child’s expected intake. Our calculations identified scenarios in which a child could consume the products and have acceptable metal exposures, defined as intakes below relevant health benchmarks. This was most evident for products with the lowest reported metal concentrations. However, in the absence of market share and consumption surveys, it remains unclear what proportion of products available to or typically consumed by children corresponds to these lower concentrations.
We also identified scenarios in which estimated dietary exposures exceeded certain health benchmarks. It is uncertain, however, whether these exceedances reflect a true health concern or instead result from conservative intake assumptions. Additionally, it is unclear how representative the evaluated dataset is of baby foods currently available on the market or how likely it is that products with higher metal concentrations would be consumed at the assumed intake levels. Of the 39 food manufacturers reviewed by Consumer Reports, we were only able to review testing data for nine brands. Despite these uncertainties, the findings are informative for hypothesis generation. Identifying a subset of products with the potential to exceed benchmarks enables prioritization of further investigation. At this stage, however, it would be premature to conclude that consumption of these products poses a population-level health risk without additional data on actual intake mass, consumption frequency, and the applicability of the selected health benchmarks to young children. Further research should also evaluate feasible alternative foods, which likely also contain non-zero concentrations of these metals.
Importantly, when assuming metal concentrations equivalent to 6 ppb (i.e. the maximum allowable LOD), some benchmark exceedances were observed. A concentration reported as ‘below the LOD’ may fall anywhere between zero and the reported LOD. In practice, caregivers who review these test results may preferentially select baby food products reported as below the LOD under the potentially incorrect assumption that these products contain no, or only negligible amounts of heavy metals and thus pose no health risk. However, this ‘below the LOD’ designation is too ambiguous to justify this conclusion when the LOD may be as high as 6 ppb. Because many manufacturers are capable of detecting metals at concentrations below this threshold, we encourage continued reporting of measured concentrations below 6 ppb and clear disclosure of the analytical LOD alongside test results, particularly when lower LODs are achieved.
Challenges and data gaps
Several factors complicate precise exposure assessment, and important data gaps remain. Reported heavy metal concentrations exhibit substantial variability and the distribution of concentrations in the marketplace is unclear, which restricts our understanding of the likelihood that a product with higher metal concentrations will be consumed. At the same time, the range of reported concentrations also indicates that it is possible to produce baby foods with lower metal concentrations.
Interpretation of these data is further complicated by inconsistent reporting of LODs. Many manufacturers do not disclose their LODs, which may be as high as 6 ppb and can, in some cases, exceed reported detected concentrations. When LODs are undisclosed and vary across laboratories, meaningful comparisons across brands become difficult. Importantly, if a food item is assumed to contain lead or mercury at the allowable LOD of 6 ppb, consumption of a single pouch-size serving (113 g) would exceed the OEHHA Proposition 65 benchmarks. Grouping truly non-detectable, potentially detectable, and absent concentrations under a single ‘<LOD’ designation therefore obscures potentially meaningful differences in risk. This lack of specificity is confusing for caregivers and does not support informed purchasing decisions.
Additional uncertainty arises from limited information on how many of these food items children typically consume per day, as well as variability in intake over time and between individuals. Parker et al.21 similarly evaluated potential health risks from arsenic, lead, cadmium, and mercury in baby foods, and estimated intake using EPA consumption data for single-ingredient foods (i.e. fruit, root vegetables, and grains). In contrast, nearly all products included in the present analysis are mixed-ingredient blends (i.e. fruit and grain or fruit and root vegetable), for which intake estimates are not readily available through commonly relied upon food intake sources (e.g. NHANES; US EPA). It is also unclear what portion of a child’s diet typically consists of packaged foods versus fresh or home-prepared foods, and likely varies inter-individually and temporally (i.e. from child to child and day to day). Evaluating a child’s complete dietary exposure to metals is therefore essential for understanding how total exposure compares to health benchmarks. In addition, some of these products may be consumed by younger children (4–12 months of age), indicating a need for further research to characterize intake patterns and exposures across early life stages.
Risk is typically evaluated relative to available alternatives. While this analysis compared estimated exposures to established health benchmarks, it is also important for caregivers and other stakeholders to recognize that alternative foods, including other packaged products, home-prepared foods, and raw ingredients, may also contain detectable concentrations of these metals. Rejecting certain foods based on reported concentration and substituting products whose metal content has not been evaluated, but is assumed to be low, will not necessarily reduce health risk.
Strengths and limitations
This analysis demonstrates how testing results reported by baby food manufacturers can be analyzed and interpreted to support informed decision-making by caregivers. We illustrate how, in the absence of more precise inputs, a caregiver or other stakeholders might incorrectly conclude that consumption of a product poses either an unacceptable or an acceptable health risk. Accurate interpretation of detection data is therefore a critical component of determining whether a potential health concern exists.
Our hypothesis-generating analysis evaluated a range of scenarios, including lower- and upper-bound metal concentrations, snack-, pouch-, and meal-size food items, consumption of multiple items per day, and comparison across multiple health benchmarks. Together, these scenarios help identify higher exposure conditions that may warrant prioritization in future research. Although we did not evaluate combined consumption of multiple item types in a single day (e.g. five snacks and three meals per day), which would increase daily exposure, the methodology presented here could be readily applied to more refined exposure analyses.
The primary limitation of this analysis is the lack of market share data for individual food products. As a result, it was not possible to estimate the likelihood that a consumer would purchase a product with a non-detectable metal concentration versus one with the highest reported concentration. Consequently, the probability that a child’s exposure would fall below or exceed a health benchmark remains uncertain, and the implications for population health remain unclear. In addition, although the Consumer Reports review identified 39 baby food brands, we were only able to access testing data for nine of these brands. It is therefore unclear whether the concentrations evaluated here are representative of all baby foods currently available to US consumers.
Another limitation is that relative market share information for individual products was not available; therefore, the likelihood of ingesting a specific product or reported concentration could not be determined. While it is also unclear how representative this subset of samples is of the available and most commonly consumed baby food products (i.e. the distribution of concentrations in our sample may not match the distribution of concentrations of all available or commonly consumed products), these results do reflect known metal concentrations in products available for sale that could be consumed by children.
CONCLUSIONS
Recent regulatory changes require baby food manufacturers to publish heavy metal detection results and make these data available to consumers. We reviewed manufacturer-reported data to evaluate the potential for health risk associated with consuming these products. Our analysis indicates that, although there are scenarios in which children could consume baby foods daily without an anticipated increase in health risk, certain products and intake patterns (e.g. four food items per day) may warrant further investigation. These findings suggest that the availability of testing results alone may be insufficient to support informed, risk-based consumer decision-making regarding product safety.