

INTRODUCTION
Artisanal and small-scale gold mine workers face significant respiratory health risks from exposure to crystalline silica dust and other particulates during mining and ore processing1. Chronic exposure to mine dust is associated with increased incidence of pneumoconiosis, chronic obstructive pulmonary disease (COPD) and silicosis2. Global studies show that the prevalence of impaired lung function in mine workers reaches 22–37%, with variations depending on exposure intensity and duration of work3.
In Indonesia, the artisanal gold mining sector involves more than one million workers, but epidemiological studies on the impact of mine dust on respiratory health are limited4. Research in Tatelu village, Minahasa, indicates minimally ventilated work practices and inadequate use of respiratory protective equipment5, but there are no quantitative studies measuring the direct relationship between dust exposure parameters and lung function in this region. International literature also shows gaps in characterizing the impact of cumulative dust exposure (accumulated duration of work) versus daily exposure (ambient concentrations) on patterns of lung function decline6.
Based on these knowledge gaps, this study aimed to examine the association between estimated daily and cumulative dust exposure and pulmonary function among artisanal gold mine workers in Tatelu village, North Sulawesi, Indonesia.
METHODS
Study design and settings
The study used a cross-sectional design according to STROBE reporting guidelines7. Data collection was conducted from April to June 2025 at an artisanal gold mining site in Tatelu village, North Minahasa Regency, North Sulawesi, Indonesia. The study site was selected due to intensive mining activities and reports of respiratory complaints among workers from the local primary health center.
Participants
The study population consisted of artisanal gold mine workers who were directly exposed to mine dust during daily work activities. Inclusion criteria were: 1) active gold mine workers with at least one year of work experience, 2) aged 18–55 years; and 3) willingness to participate as indicated by written informed consent. Exclusion criteria included: 1) a prior physician-diagnosed history of asthma or chronic obstructive pulmonary disease (COPD) before employment in mining, 2) congenital thoracic abnormalities, and 3) acute respiratory infection within two weeks prior to data collection. Of the 35 workers who met the eligibility criteria, 30 agreed to participate, resulting in a response rate of 85.7%.
Variables and measurements
Dependent variable
Pulmonary function was assessed using a portable spirometer (MIR Spirobank II) operated by trained health personnel in accordance following ATS/ERS standards8. Parameters included forced vital capacity (FVC) and forced expiratory volume in 1 second (FEV1) in percentage prediction based on a reference Asian population9. Pulmonary function was classified as abnormal when FVC or FEV1 was less than 80% of the predicted.
Independent variables
These included daily dust exposure estimated using an indirect calculation approach based on dust concentration, inhalation rate and working duration. Median dust concentration (C) was obtained from environmental measurements conducted over two working days and expressed in mg/m³. The inhalation rate (IR) was derived from published literature (25.06 ± 4.33 m³/hour)10. Individual working hours per day (T) were obtained through structured interviews.
Daily dust exposure (PDH) was calculated using the following formula: PDH=C×IR×T. Cumulative dust exposure (PDK) was estimated by multiplying daily dust exposure by the number of working days per year (365 days) and total years of employment:
PDK=PDH×365×years of employment.
Covariates
Potential confounding variables included age (years), smoking status (number of cigarettes per day), daily working hours (categorized as ≥12 hours/day and <12 hours/day), years of employment, and use of personal protective equipment (PPE). All covariates were collected through structured face-to-face interviews.
Statistical analysis
Statistical analyses were performed using R software version 4.3.1 . Data distribution was assessed using the Shapiro–Wilk normality test. Descriptive statistics were presented as mean ± standard deviation for normally distributed variables, or median and interquartile range (IQR) for non-normally distributed variables. Associations between dust exposure variables and pulmonary function parameters were examined using Pearson or Spearman correlation tests as appropriate. Multivariable linear regression analyses were conducted to evaluate the association between daily and cumulative dust exposure and pulmonary function outcomes (FEV1 and FVC), adjusting for age, smoking intensity, and daily working hours. Regression coefficients (β) with 95% confidence intervals were reported. Statistical significance was defined as p<0.05.
RESULTS
A total of 30 artisanal gold mine workers from Tatelu village, North Minahasa Regency, North Sulawesi, Indonesia was included in the analysis. The descriptive characteristics of the study participants, dust exposure variables, and pulmonary function parameters are summarized in Table 1. The median age of the participants was 31.5 years (IQR: 25.5–39.2), with a median employment duration of 5.5 years (IQR: 3.2–9.0). The median daily working duration was 12.0 hours (IQR: 8.0–12.0). Almost all participants were smokers (97%), with a median cigarette consumption of 15 cigarettes per day (IQR: 12–16). The median estimated daily dust exposure was 9.4 mg (IQR: 6.3–11.7). The median cumulative dust exposure was 18.8×10³ mg (IQR: 10.5–32.7).
Table 1
Characteristics, dust exposure, and pulmonary test of artisanal gold mine workers in Tatelu village, North Sulawesi, Indonesia, April–June 2025 (N=30)
Pulmonary function assessment showed that 21 participants (70%) had an FVC value <80% of the predicted value, while 16 participants (53%) had an FEV1 value <80%. The mean FVC was 72.9% (SD=12.4), and the median FEV1 was 79.0% (IQR: 72.2–84.5). The mean FEV1/FVC ratio was 1.1 (SD=0.1).
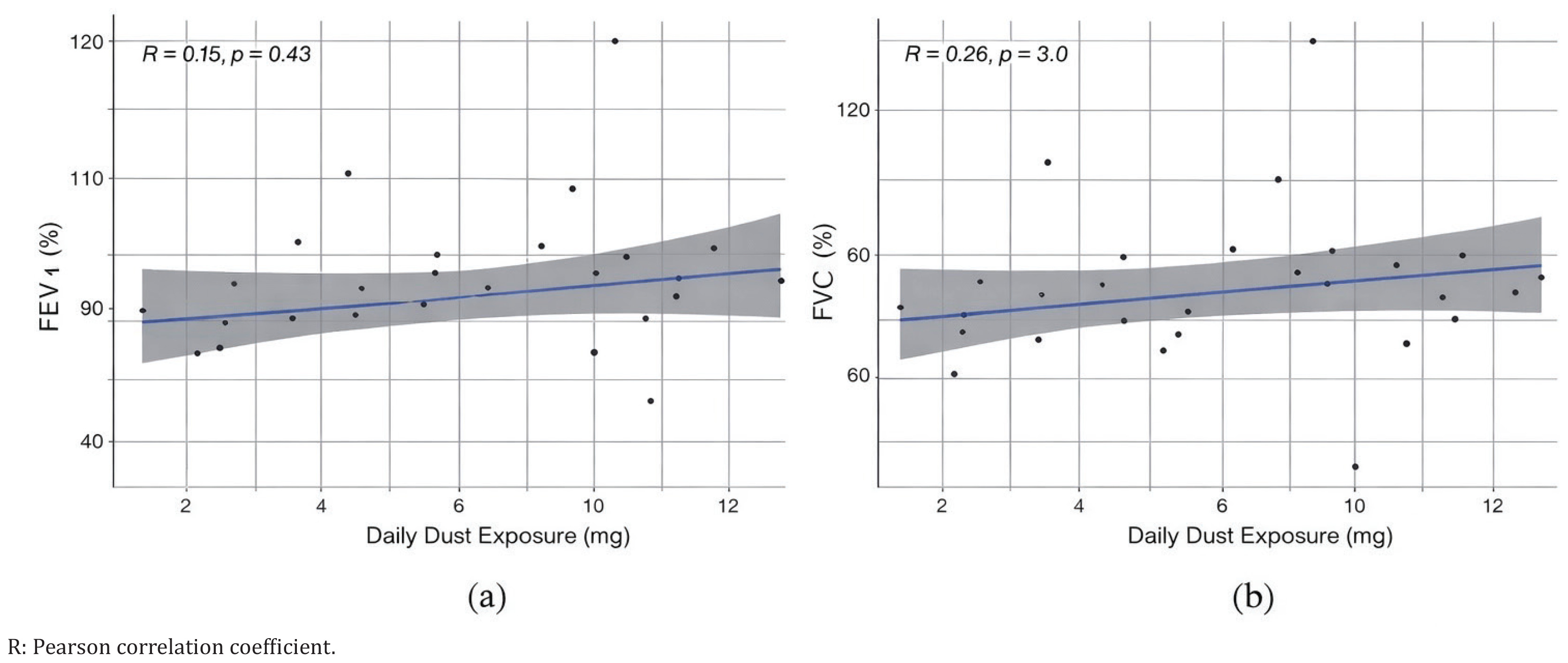
Correlation analyses between dust exposure variables and pulmonary function parameters are presented in Figures 1 and 2. Pearson correlation coefficients indicated weak associations between daily dust exposure and FEV1 (r=0.15) and FVC (r=0.20). Cumulative dust exposure showed near-zero correlation with both FEV1 and FVC.

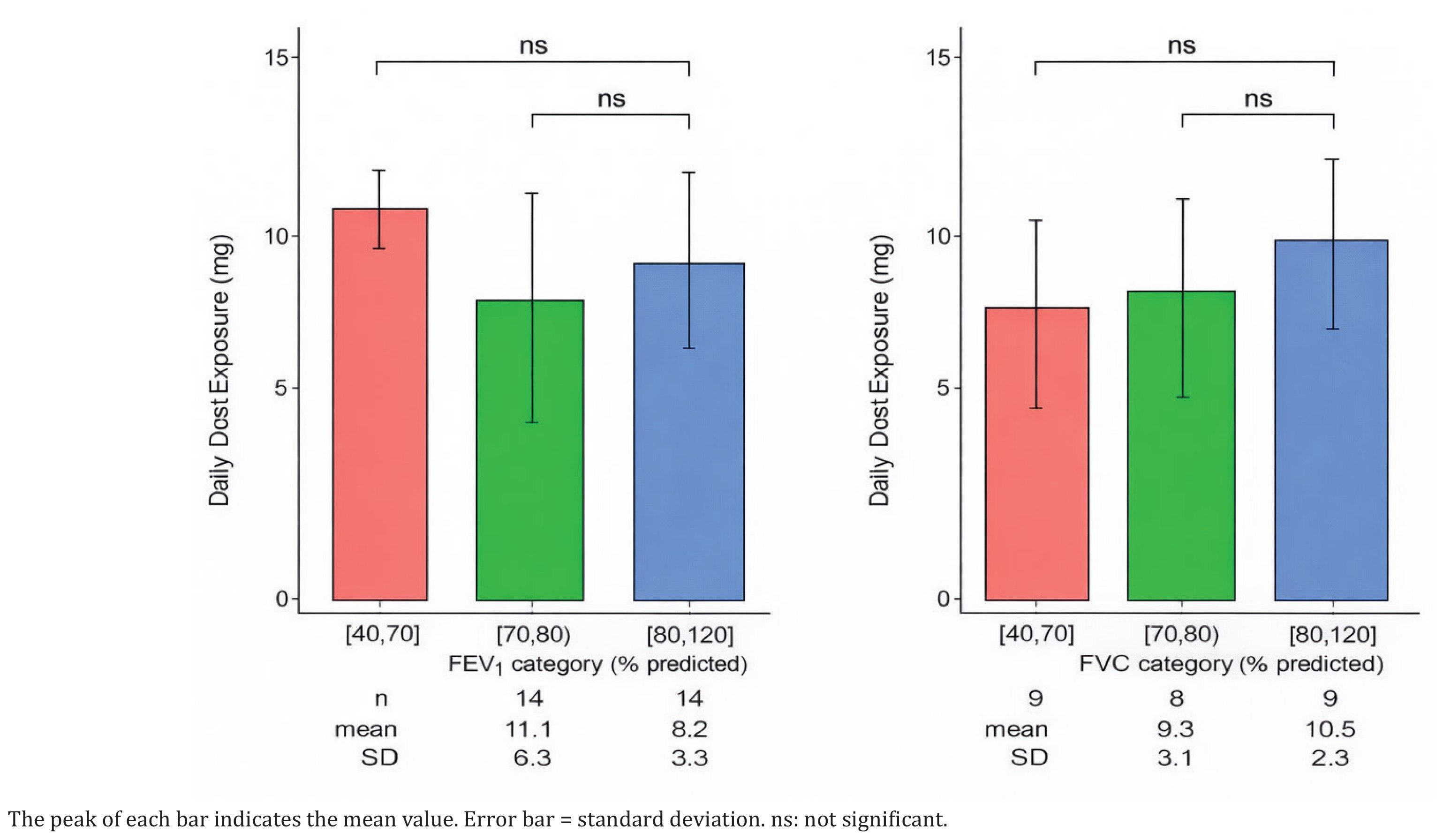
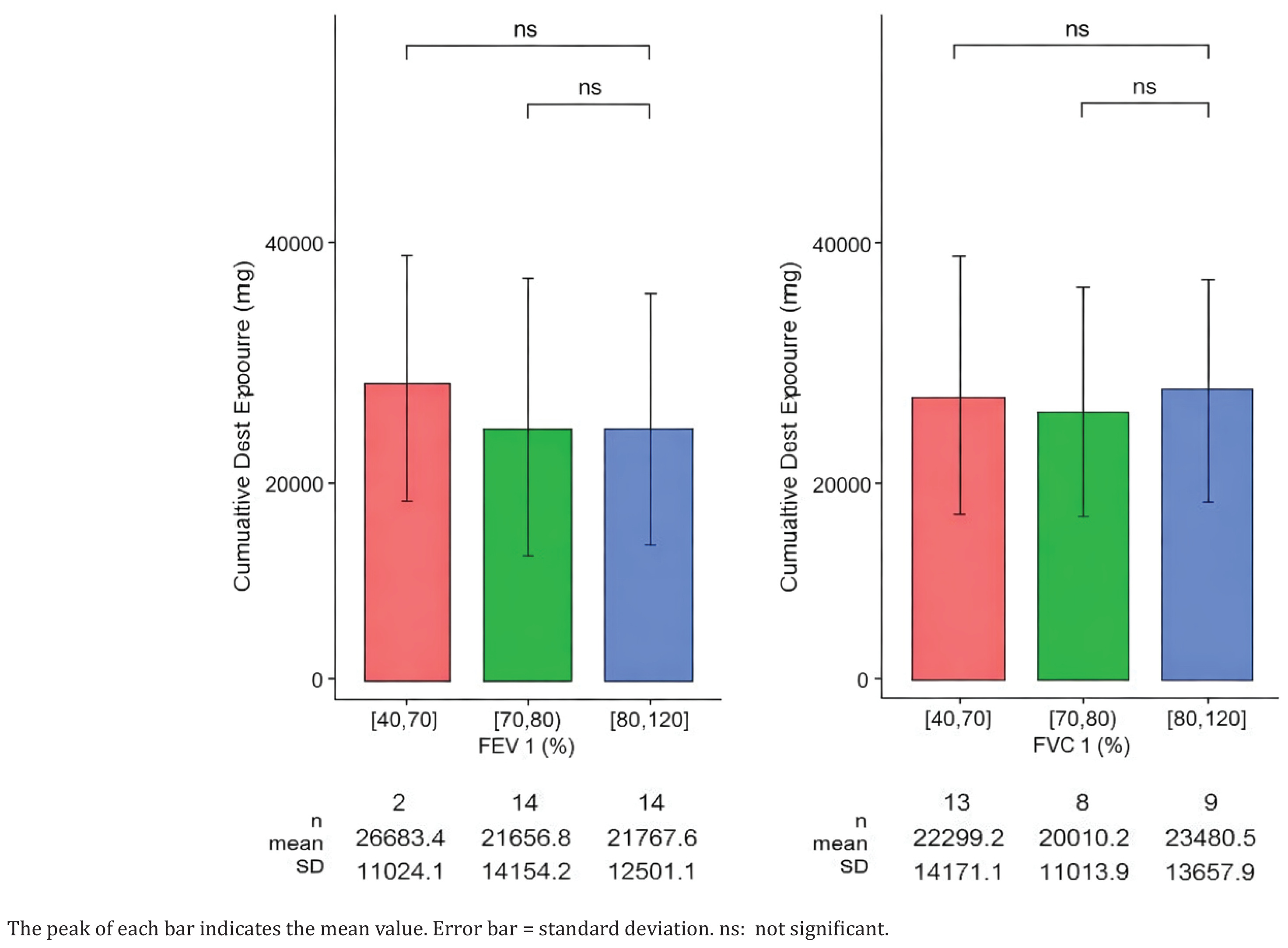
The distribution of daily and cumulative dust exposure according to pulmonary function categories is illustrated in Figures 3 and 4. Mean daily dust exposure values across FEV1 and FVC categories showed overlapping distributions. No marked separation was observed between exposure levels among workers with normal and abnormal pulmonary function categories.
One component of the dust exposure calculation is the number of working hours per day of each study subject. This information was obtained through interviews with the sample, rather than observation for direct calculation. Further evaluation suggests that the number of hours worked is more indicative of the fitness of the miners in the sample than the quantity of dust exposure. Figure 5 shows that workers with daily working hours of ≥12 hours tend to have better pulmonary function test results, which is particularly evident for FVC.
Figure 5
Distribution of pulmonary function test results according to individual working hour categories
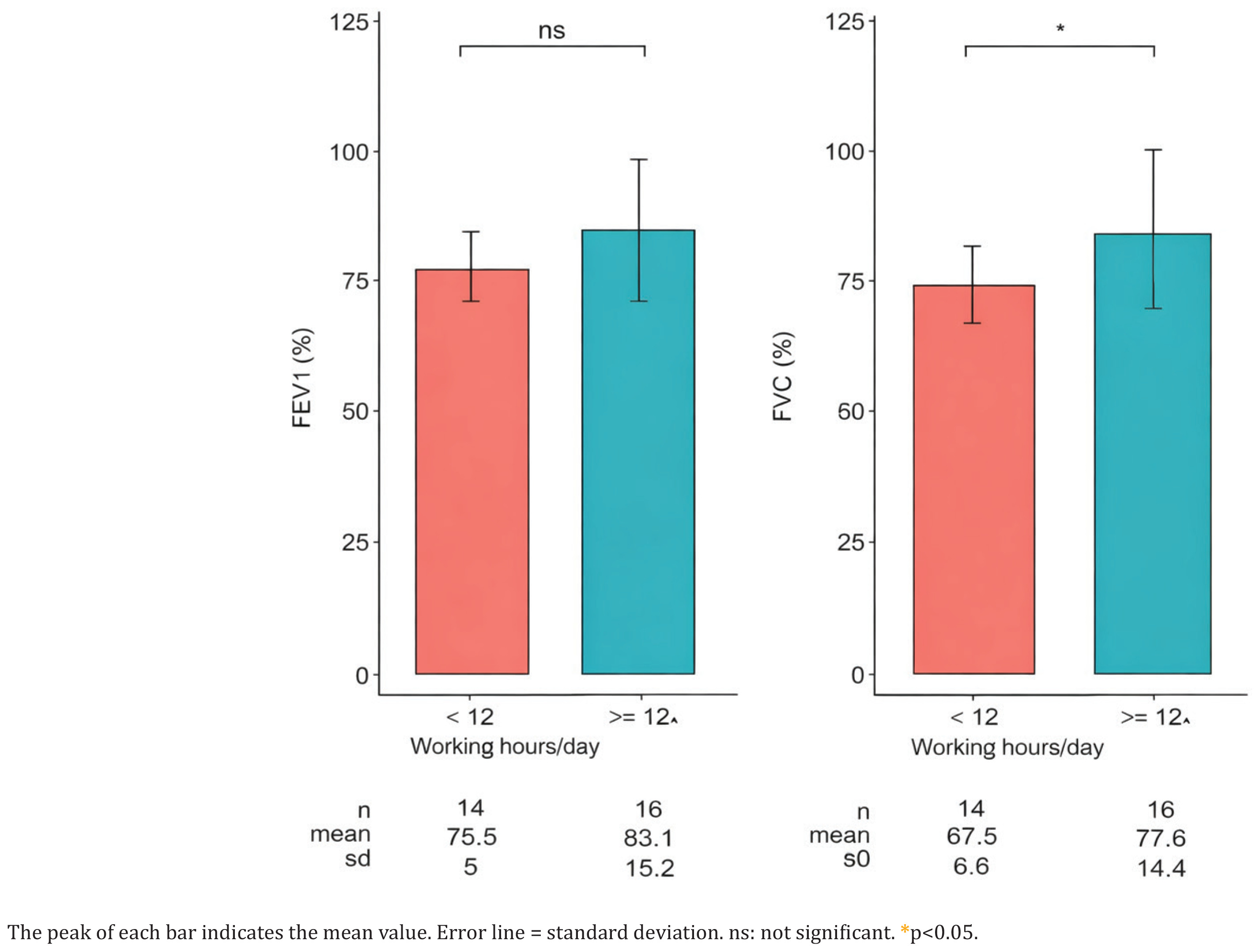
Results of multivariable linear regression analyses are presented in Table 2. After adjustment for age, smoking intensity, and daily working hours, neither daily nor cumulative dust exposure showed statistically significant associations with FEV1 or FVC. Workers who reported working ≥12 hours per day had higher adjusted FVC values compared with those working <12 hours per day (β=10.12; 95% CI: 1.53–18.72).
Table 2
Multivariable linear regression analysis of factors associated with pulmonary function parameters among artisanal gold mine workers in Tatelu village, North Sulawesi, Indonesia, April–June 2025
DISCUSSION
This study examined the association between daily and cumulative dust exposure and pulmonary function among artisanal gold mine workers in Tatelu village, North Sulawesi. Overall, the findings did not demonstrate a statistically significant association between estimated dust exposure and pulmonary function parameters (FEV1 and FVC). However, longer daily working hours were associated with higher FVC values after adjustment for potential confounders.
The absence of a clear association between dust exposure and pulmonary function in this study contrasts with findings from studies conducted in large-scale mining settings, where higher dust exposure levels are more consistently associated with reduced lung function1. One possible explanation is that the estimated dust exposure levels in this population may have been below the threshold required to produce measurable impairment in pulmonary function. The weak positive trend observed between daily dust exposure and pulmonary function parameters may reflect a healthy worker effect, whereby individuals with better baseline health or physical fitness are more likely to tolerate longer working hours and higher exposure levels. Similar patterns have been reported in occupational studies where physically fitter workers remain employed in more demanding tasks, while less healthy workers leave the workforce earlier11.
Several methodological factors may have influenced the observed findings. Dust concentration measurements were limited to two working days and therefore may not fully capture daily, weekly, or seasonal variability in exposure. In addition, inhalation rates were obtained from the literature rather than measured individually, which may have introduced exposure misclassification. Working hours and employment duration were collected through self-report, increasing the potential for recall bias. These sources of non-differential misclassification may have attenuated the magnitude of associations between dust exposure and pulmonary function outcomes.
Previous studies among miners and other dust-exposed occupational groups have generally reported inverse associations between dust exposure and lung function decline2. However, the strength and direction of these associations vary depending on exposure intensity, duration, and study design. Studies conducted in artisanal or small-scale mining settings have reported heterogeneous results, reflecting differences in work practices, environmental controls, and worker characteristics. The findings of the present study contribute to the limited body of evidence on dust exposure and respiratory health in artisanal gold mining populations in Indonesia, an occupational group that remains under-represented in epidemiological research.
Future studies should prioritize improved exposure assessment through repeated and personal dust monitoring and incorporate longitudinal designs to better characterize changes in pulmonary function over time. Studies with larger sample sizes and more comprehensive control of potential confounders may provide clearer insights into the relationship between dust exposure and respiratory health in artisanal mining settings.
Strengths and limitation
A key strength of this study is the use of a quantitative approach to estimate both daily and cumulative dust exposure using concentration, inhalation rate, and working time parameters. The study also employed standardized spirometry measurements in accordance with international guidelines. Nevertheless, several limitations should be acknowledged. The cross-sectional design precludes causal inference between dust exposure and pulmonary function outcomes. The small sample size limited statistical power to detect modest associations. Pulmonary function was assessed at a single time point, which may not reflect longitudinal changes. Additionally, residual confounding from unmeasured factors such as nutritional status, co-exposure to other occupational hazards, and detailed assessment of personal protective equipment use, cannot be excluded.
CONCLUSIONS
This study found no statistically significant association between estimated daily and cumulative dust exposure and pulmonary function among artisanal gold mine workers in Tatelu village, North Sulawesi. However, longer daily working hours were associated with higher FVC values. These findings highlight the complexity of occupational exposure and respiratory health in artisanal mining settings and underscore the need for further research using improved exposure assessment and longitudinal study designs.