

INTRODUCTION
Secondhand smoke (SHS), also known as passive or involuntary smoking, remains a major global health concern despite declines in active smoking in many regions. Tobacco smoke contains thousands of chemicals, including numerous carcinogens and cardiorespiratory toxins, and SHS exposure has been causally linked to ischemic heart disease, stroke, lung cancer, chronic obstructive pulmonary disease, asthma, lower respiratory infections, otitis media, and other conditions in both adults and children1-3. Recent burdenofdisease analyses estimate that SHS exposure contributed to approximately 1.3 million premature deaths worldwide in 2019, with tens of thousands of these occurring in children aged <14 years1,2,4. Children and adolescents are disproportionately affected, especially in low and middleincome countries where smokefree protections are weaker and household smoking is more common2,4,5.
Global surveillance data underscore the magnitude of adolescent SHS exposure. Analysis of Global Youth Tobacco Survey (GYTS) data from more than 140 countries suggests that roughly onethird of adolescents are exposed to SHS at home, and over half in public places4. However, these overall estimates mask substantial regional inequalities. Systematic reviews highlight that estimates for African and other lowresource settings are often sparse, methodologically heterogeneous, or entirely absent, limiting reliable assessment of SHSattributable disease burden1,5. Serum cotinine studies further show that selfreported exposure frequently underestimates true SHS levels in children, complicating burden estimates and hampering policy evaluation3,6.
SubSaharan Africa is undergoing a tobacco transition: historically low smoking prevalence is threatened by aggressive marketing, demographic change, and uneven implementation of the WHO Framework Convention on Tobacco Control (FCTC)6,7. Adult smoking prevalence in several countries, including Zambia, remains modest in absolute terms but is high within specific male and socioeconomic subgroups5. In such contexts, adolescents may experience substantial SHS exposure in homes, schools, public transport, hospitality venues, and increasingly through emerging products such as waterpipes and electronic cigarettes, which are often weakly regulated and perceived as less harmful. Yet, compared with evidence from Asia, Europe, and North America, there are few nationally representative data describing the prevalence and determinants of adolescent SHS exposure in African settings1,4,5.
Understanding the associations of SHS exposure in adolescence is critical because this developmental period is marked by heightened vulnerability of the brain and lungs to nicotine and tobacco toxicants, as well as the consolidation of longterm health behaviors3,8. Repeated SHS exposure in childhood and adolescence impairs lung growth, increases the risk of wheezing and asthma, and contributes to cardiometabolic and blood pressure changes that may track into adulthood2,3. At the same time, SHS often cooccurs with powerful social influences, parental and peer smoking, school and neighborhood norms, and ubiquitous tobacco marketing, that increase the likelihood of smoking initiation and progression to regular use4,9,10. Identifying sociodemographic, household, school, peer, and media factors associated with SHS exposure may help improve understanding of the contexts in which adolescents experience exposure and inform future research and policy discussions4,7,9,11.
To our knowledge, few studies have examined the prevalence and associations of SHS exposure among nationally representative samples of in-school adolescents in Zambia12. This study addresses that gap by estimating the burden of SHS exposure and examining its demographic, behavioral, social, and environmental determinants, thereby providing evidence on the prevalence and correlates of SHS exposure among adolescents in Zambia.
METHODS
Data management
The study used data from the 2021 Zambia Global Youth Tobacco Survey (GYTS) to conduct the analysis. The GYTS is a nationally representative, school-based, cross-sectional survey that employs a self-administered questionnaire to monitor tobacco use and related behaviors among adolescents. In Zambia, the survey was administered in grades 7–9 (primarily ages 11–17 years). A total of 6499 students completed the survey (overall response rate of 75.7%)13.
Outcome variables
The primary outcome was SHS exposure. Binary indicators were created for SHS exposure across four settings using standard GYTS questionnaire items14. SHS exposure at home was defined as any reported days in the past seven days during which someone smoked in the student’s presence inside the home14. SHS exposure in enclosed public places was defined as any reported days in the past seven days that someone smoked in the student’s presence inside an enclosed public place, such as shops or restaurants, excluding the home. SHS exposure in outdoor public places was defined as any reported days in the past seven days during which someone smoked in the student’s presence in outdoor public areas such as playgrounds, sidewalks, or parks. SHS exposure at school was defined as any reported sighting of someone smoking inside school buildings or on school property in the past 30 days. Each setting was coded as 1 for any exposure and 0 for no exposure. A composite binary variable was also created to indicate exposure in any of the four settings.
Predictor variables
The study examined a comprehensive set of predictor variables organized by socio-ecological level. Each predictor was coded as specified, with reference categories indicated where applicable, consistent with standard GYTS measures and previous analyses of this dataset13. The study examined a comprehensive set of predictor variables organized according to the socio-ecological framework. Individual-level factors included demographic characteristics such as age (11–17 years), sex (male, female), and grade level (7–9). Socio-economic status was assessed using a wealth index derived from reported weekly spending money and categorized into tertiles (low, middle, and high). Tobacco-related behaviors included ever trying cigarette smoking, current cigarette use, use of hand-rolled cigarettes, ever tried shisha, and awareness of electronic cigarettes. Knowledge and attitudes were assessed using beliefs about long-term tobacco use causing cancer and leading to drug use, while future intentions included intention to use tobacco in the next 12 months, as per the standard WHO GYTS questionnaire.
Interpersonal-level factors included family and peer influences. These comprised parental or guardian smoking in the home, father smoking status, and whether close friends smoked tobacco. School environment factors included teacher smoking and observations of teachers smoking on school grounds. Environmental and media factors included exposure to tobacco-related media and marketing, such as seeing people using tobacco on television, exposure to tobacco advertisements, ownership of tobacco-branded items, and exposure to anti-tobacco messages through television, radio, or social media. Policy and education factors included whether students had been taught about the dangers of tobacco use during the past year. Geographical factors included region of residence, categorized as Lusaka, Rest of Country (ROC), and tobacco-growing regions.
Statistical analysis
Data management was done in R version 4.5.215,16. All predictor variables were created according to the same definitions and coding schemes used in prior work to ensure consistency across analyses. Descriptive analyses were conducted to summarize the characteristics of study participants, with results presented as frequencies and survey-weighted percentages. The weighted prevalence of SHS exposure was estimated overall and across levels of each predictor variable. All prevalence estimates were accompanied by 95% confidence intervals (CIs) calculated using survey-adjusted methods to account for the complex sampling design of the GYTS.
Pairwise comparisons were assessed using weighted prevalence estimates and corresponding confidence intervals, while adjusted associations were examined using multivariable logistic regression models. Crude odds ratios were not presented to avoid redundancy. Survey-weighted logistic regression models were fitted separately for each predictor, and adjusted odds ratios (AORs) with corresponding 95% confidence intervals (CIs) and p-values are reported with statistical significance assessed at the 5% level17,18. These analyses provided an initial assessment of factors associated with SHS exposure while appropriately incorporating sampling weights, stratification, and clustering. In multivariable models, certain variables (region, age, sex, and grade) were included a priori as potential confounding factors, regardless of statistical significance, to control for demographic differences and improve model validity19. A survey-adjusted logistic regression model including all candidate predictors was fitted to obtain the final adjusted model19.
Ethics
This study was conducted in accordance with internationally accepted ethical standards for research involving human participants. Access to the anonymized 2021 GYTS dataset was obtained through the World Health Organization (WHO) NCD Microdata Repository. The GYTS data are fully de-identified prior to release, ensuring that no individual respondents can be identified. As the analysis involved secondary use of existing anonymized data and required no direct contact with participants, additional ethical approval and informed consent were not required. The study therefore posed minimal risk and complied with WHO data access and research ethics requirements.
RESULTS
Descriptive analysis
Table 1 presents the characteristics of the study sample comprising 6499 adolescents aged 11–17 years from three regions in Zambia: Lusaka (n=2027), the Rest of the Country (ROC; n=2500), and Tobacco Regions (n=1972). The age distribution was centered on mid-adolescence, with 25% (n=1589) aged 14 years and 21% (n=1363) aged 15 years. Adolescents aged 11 years constituted 4.1% (n=265), while those aged 17 years accounted for 11% (n=678). Females comprised 57% (n=3681) of the sample, and males 43% (n=2725). Students were evenly distributed across grades, with 35% in Grade 7, 32% in Grade 8, and 33% in Grade 9.
Table 1
Characteristics of school-going adolescents in Zambia, 2021 Global Youth Tobacco Survey (N=6499)
Tobacco-related behaviors differed significantly by region (Table 1). Overall, 21% (n=1083) of students had ever tried cigarette smoking, with prevalence highest in Tobacco Regions (32%), followed by ROC (20%) and Lusaka (14%) (p<0.001). Current cigarette smoking showed a similar pattern, reported by 26% of students in Tobacco Regions, 16% in ROC, and 7.5% in Lusaka (p<0.001). Household tobacco exposure also varied regionally; parental smoking at home was reported by 16% overall, ranging from 12% in Lusaka to 19% in Tobacco Regions (p<0.001).
School-based tobacco exposure was common. Overall, 14% of students reported seeing teachers smoking at school, and 14% reported teachers actually smoking at school, with both measures significantly higher in Tobacco Regions than in Lusaka or ROC (p<0.001). Social influences were also prevalent, with 25% reporting friends who smoke tobacco. Exposure to anti-tobacco media messages was reported by 62% of students overall and did not differ meaningfully by region, while 47% reported having been taught about the dangers of tobacco use.
Socioeconomic indicators showed that 53% of students were classified as low wealth, 18% as middle wealth, and 29% as rich. Regarding spending money, 21% reported having none, while 32% reported low, 27% medium, and 20% high spending money.
Prevalence of any SHS exposure
Table 2 presents the weighted prevalence of any SHS exposure. Overall, 66.0% of adolescents experienced SHS exposure. Prevalence was highest among younger adolescents (77.7%) and declined through mid-adolescence before rising modestly among 17-year-olds (69.4%). SHS exposure did not differ by sex and varied only slightly by grade level.
Table 2
Weighted prevalence of exposure to secondhand smoking among school-going adolescents in Zambia, 2021 Global Youth Tobacco Survey (N=6499)
Strong gradients were observed across tobacco-related behaviors. Adolescents who had ever tried cigarette smoking reported substantially higher SHS exposure (79.5%) compared with those who had not (60.2%). Exposure was even higher among current cigarette smokers (90.9%) and users of hand-rolled cigarettes (87.2%).
Household and social environments were strongly associated with SHS exposure. Adolescents whose parents or guardians smoked in the home experienced SHS exposure at a prevalence of 88.2%, compared with 62.6% among those without household smoking. Similarly, 84.1% of students with friends who smoke reported SHS exposure, compared with 61.0% among those without smoking friends. Observing teachers smoking at school was associated with SHS exposure prevalence exceeding 85%.
Media exposure showed consistent associations. Adolescents who reported seeing people use tobacco on television had higher SHS exposure (74.7%) than those who did not (60.3%), and exposure to tobacco advertisements was associated with a prevalence of 79.4%. On the other hand, exposure to anti-tobacco media messages and being taught about the dangers of tobacco use were also associated with higher SHS exposure. Regional differences in SHS exposure were modest, with prevalence ranging from 65.7% in ROC to 67.9% in Lusaka. Higher wealth and greater access to spending money were associated with slightly higher SHS exposure.
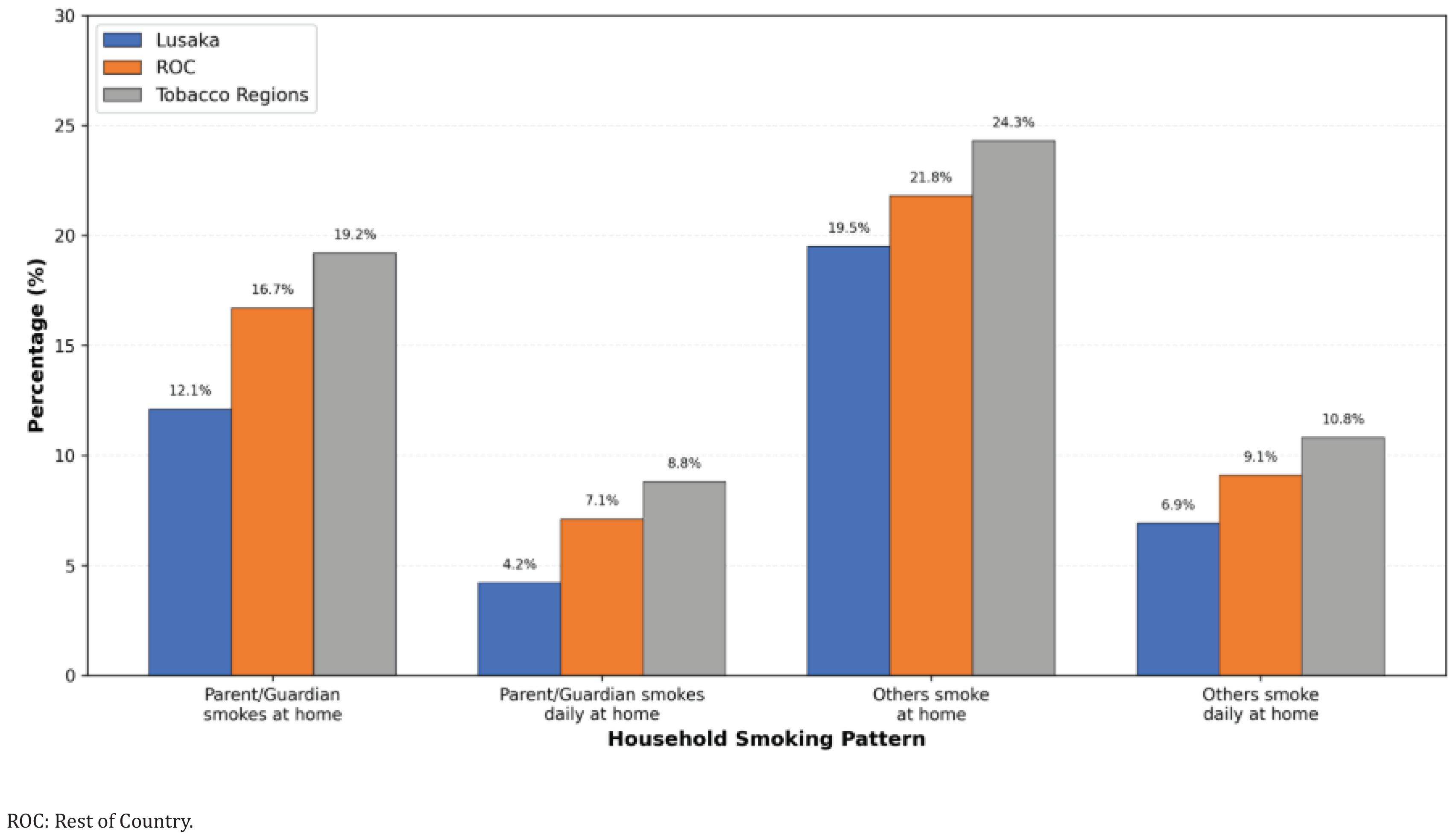
Household smoking patterns
Figure 1 summarizes household smoking patterns by region. Overall, 16.0% of adolescents reported that a parent or guardian smokes at home, and 6.7% reported daily parental smoking. Smoking by other household members was more common, reported by 21.8% overall, with daily smoking by others reported by 8.9%. All household smoking indicators were more prevalent in Tobacco Regions than in Lusaka
Factors associated with exposure to SHS
Figure 2 presents results from the multivariable logistic regression analysis examining factors associated with any SHS exposure among adolescents. All estimates are adjusted for demographic, social, environmental, and socio-economic factors, holding all other variables constant. The geographical region was significantly associated with SHS exposure. Compared with Lusaka, students living in the Rest of the Country (ROC) had lower odds of SHS exposure (AOR=0.81; 95% CI: 0.69–0.95, p=0.011). Adolescents in Tobacco Regions also had reduced odds compared with Lusaka (AOR=0.68; 95% CI: 0.57–0.81, p<0.001). Age was not independently associated with SHS exposure after adjustment. Compared with younger adolescents, 12-year-olds had slightly higher odds (AOR=1.05; 95% CI: 0.62–1.76, p=0.854), while adolescents aged 13–17 years generally showed lower odds, ranging from AOR=0.91 among those aged 13 years (95% CI: 0.56–1.47, p=0.701) to AOR=0.86 among those aged 14 years (95% CI: 0.53–1.37, p=0.523). However, none of these associations was statistically significant, and all confidence intervals included one, suggesting that the observed age differences may be due to chance rather than true age-related effects.
Figure 2
Factors associated with secondhand smoke (SHS) exposure by school-going adolescents in Zambia, 2021 Global Youth Tobacco Survey (N=6499)
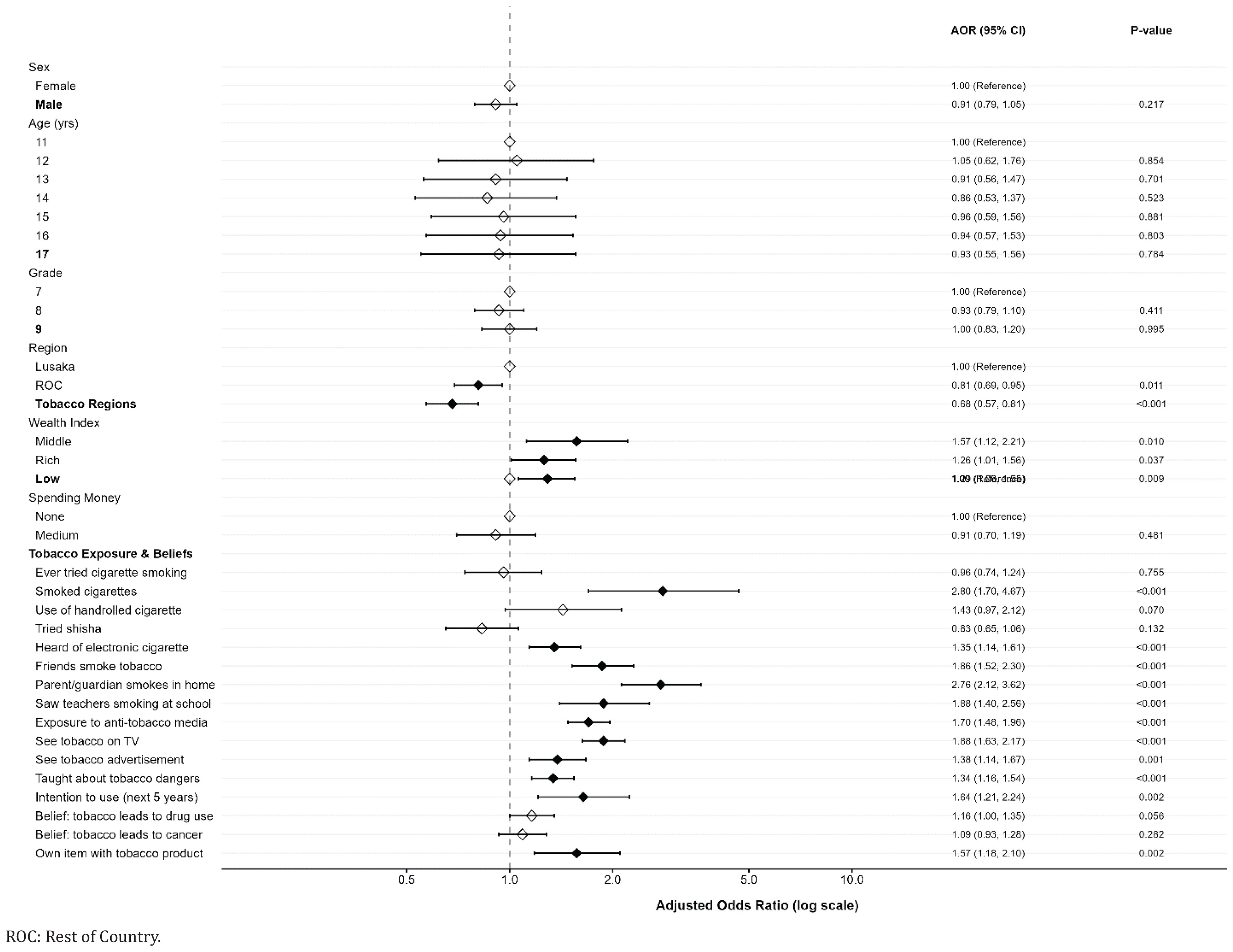
Sex was also not associated with SHS exposure. Males had similar odds compared with females (AOR=0.91; 95% CI: 0.79–1.05, p=0.217). Grade level showed no meaningful association, with Grade 8 students having slightly reduced odds compared with Grade 7 (AOR=0.93; 95% CI: 0.79–1.10, p=0.411), and Grade 9 students showing no difference (AOR=1.00; 95% CI: 0.83–1.20, p=0.995). Exposure to anti-tobacco interventions was positively associated with SHS exposure. Adolescents who reported exposure to anti-tobacco media messages had higher odds of reporting SHS exposure (AOR=1.70; 95% CI: 1.48–1.96, p<0.001). Similarly, those who had been taught about the dangers of tobacco use had increased odds (AOR=1.34; 95% CI: 1.16–1.54, p<0.001). Social and household environments showed the strongest associations with SHS exposure. Adolescents living with a parent or guardian who smokes had markedly higher odds of SHS exposure (AOR=2.76; 95% CI: 2.12–3.62, p<0.001). Having friends who smoke tobacco was associated with substantially higher odds (AOR=1.86; 95% CI: 1.52–2.30, p<0.001). Seeing teachers smoking at school was also associated with increased odds of exposure (AOR=1.88; 95% CI: 1.40–2.56, p<0.001).
Media and commercial exposures were associated with SHS exposure. Adolescents who reported seeing people using tobacco on television had substantially higher odds of reporting SHS exposure (AOR=1.88; 95% CI: 1.63–2.17, p<0.001), while exposure to tobacco advertisements was also associated with higher odds (AOR=1.38; 95% CI: 1.14–1.67, p=0.001). Personal tobacco-related behaviors and perceptions were significantly associated with SHS exposure. Adolescents who had smoked cigarettes had higher odds of exposure (AOR=2.80; 95% CI: 1.70–4.67, p<0.001). Awareness of electronic cigarettes increased the odds (OR=1.35; 95% CI: 1.14–1.61, p<0.001), while ownership of tobacco-branded items was associated with higher odds (AOR=1.57; 95% CI: 1.18–2.10, p=0.002). Adolescents who intended to use tobacco in the next five years also had increased odds of current SHS exposure (AOR=1.64; 95% CI: 1.21–2.24, p=0.002). In contrast, having ever tried cigarette smoking was not independently associated with SHS exposure (AOR=0.96; 95% CI: 0.74–1.24, p=0.755). Tobacco-related knowledge showed mixed associations. Belief that long-term tobacco use leads to drug use showed a borderline association with SHS exposure (AOR=1.16; 95% CI: 1.00–1.35, p=0.056), while belief that tobacco use leads to cancer was not associated with SHS exposure (AOR=1.09; 95% CI: 0.93–1.28, p=0.282).
Socio-economic factors showed varying patterns. Compared with adolescents with no spending money, those with low spending money had higher odds of reporting SHS exposure (AOR=1.29; 95% CI: 1.06–1.55, p=0.009), while those with medium levels of spending money showed no association (AOR=0.91; 95% CI: 0.70–1.19, p=0.481). Compared with adolescents in the low wealth category, those in the middle wealth group had higher odds of SHS exposure (AOR=1.57; 95% CI: 1.12–2.21, p=0.010), and those in the high wealth group also showed increased odds (AOR=1.26; 95% CI: 1.01–1.56, p=0.037). Some variables were not independently estimated due to collinearity or lack of statistical significance. Trying shisha (AOR=0.83; 95% CI: 0.65–1.06, p=0.132) and use of hand-rolled cigarettes (AOR=1.43; 95% CI: 0.97–2.12, p=0.070) were also not significantly associated with SHS exposure.
DISCUSSION
SHS exposure among adolescents in Zambia was widespread and associated primarily with social and environmental factors. Exposure was strongly associated with household smoking, peer smoking, and observing teachers smoking at school. Media exposure and tobacco-related behaviors were also important predictors, while demographic characteristics such as age, sex, and grade level were not independently associated with exposure. Socio-economic factors showed mixed associations, suggesting that adolescents encounter SHS across multiple environments. These findings suggest that adolescent exposure in Zambia is associated largely with interpersonal and environmental influences rather than individual demographic characteristics.
The high level of SHS exposure observed in this study is consistent with findings from other low- and middle-income countries, where patterns of adolescent exposure vary across settings. Further research is needed to better understand how contextual differences influence exposure. Evidence from African countries and other low- and middle-income regions has indicated considerable variability in adolescent SHS exposure, reflecting differences in smoking patterns, differences in smoke-free environments, urbanization, and cultural norms surrounding tobacco use in homes, schools, and public places20-25. Such variation in prevalence across countries can be attributed to differences in adult and youth smoking rates, enforcement and coverage of smoke-free laws, urbanization, and social norms regarding tobacco use at home, school, and public places23. The relatively elevated exposure observed in this study suggests that adolescents in Zambia remain substantially exposed to tobacco smoke, highlighting the need for further studies to better understand determinants of exposure.
In Zambia, SHS exposure was highest among younger adolescents, declined through mid-adolescence, then rose again by late adolescence. However, after adjustment for confounders, age was not independently associated with SHS exposure, contrasting with studies from Cambodia, Mongolia, Taiwan, and the US that found increasing age correlated with higher SHS exposure26,27. Sex was also not a significant factor; males and females had similar odds of SHS exposure. This aligns with some Malaysian studies but contrasts with US data, where girls were more susceptible to SHS28. The lack of sex difference in Zambia may reflect local patterns of tobacco use and prevailing social norms.
Strong gradients were observed across tobacco-related behaviors. Adolescents who had ever tried cigarette smoking reported much higher SHS exposure compared to those who had not. Exposure was even higher among current cigarette smokers and users of hand-rolled cigarettes. These findings are consistent with studies from Malaysia, China, South Africa, Japan, and the US showing that adolescent smokers are more likely to be exposed to SHS, likely due to clustering within peer groups who share smoking behaviors23,24,27. Smokers tend to befriend other smokers because they share similar behaviors, and many adolescents smoke together in groups, which increases their collective exposure to SHS.
Household and social environments were strongly associated with SHS exposure. Adolescents whose parents or guardians smoked at home experienced higher SHS prevalence compared to those without household smoking, a pattern echoed across Africa, Asia, Latin America, and high-income countries21,22,26. Similarly, having friends who smoke was associated with increased SHS exposure; observing teachers smoking at school was associated with higher SHS prevalence. These results are consistent with international evidence that parental, peer, and teacher smoking are among the strongest predictors of youth SHS exposure21,22. In many settings, including The Gambia and West Africa, parental education level, living arrangements, home smoking rules, and being sent to purchase cigarettes, all significantly increase the risk of adolescent SHS exposure.
Media influences also play a significant role. Zambian adolescents who saw people use tobacco on television had higher SHS exposure than those who did not. Unexpectedly, seeing anti-tobacco media messages or being taught about tobacco dangers was also linked to higher SHS exposure, likely reflecting targeted interventions in high-exposure environments or greater recall among frequently exposed youths. Similar ‘paradoxical’ associations have been documented in West African GYTS data and pooled African analyses8.
Regional differences within Zambia were modest, with students outside Lusaka having lower odds of SHS exposure after adjustment, a pattern seen elsewhere where urbanization increases risk21. Higher wealth status and greater access to spending money were associated with slightly higher SHS exposure, a complex pattern also observed in Kuwait and Malaysia, where both low-SES home exposures and high-SES social exposures contribute24,29.
Multivariable analysis confirmed that living with a parent or guardian who smokes was associated with substantially higher odds of SHS exposure; having friends who smoke was associated with substantially higher odds; seeing teachers smoke at school was associated with considerably higher odds, media or commercial exposures remained significant predictors; personal tobacco use strongly predicted higher odds; while age, sex, grade level showed no independent association. The Zambian findings fit within a broader literature showing that where smoke-free environments are limited, and adult or peer smoking remains common, the majority of adolescents are exposed to SHS. The strong influence of family, peer, or teacher smoking has been repeatedly demonstrated across Africa, Asia, Europe, North America, Latin America, and is further reinforced by biomarker-based studies using cotinine levels that confirm self-reported exposures often underestimate true prevalence6. The association between anti-tobacco education or media messages and higher reported SHS has also been observed elsewhere, often interpreted as reverse causation or targeted messaging in high-risk settings.
Socio-economic disparities were observed. Children from low income families or rural areas are often more exposed due to crowded housing conditions or less stringent enforcement of home bans26,30, while wealthier youths may encounter more public or social exposures as seen in Hong Kong’s rising neighbor-sourced household smoke trends. Thirdhand smoke, which refers to residual nicotine on surfaces, has emerged as an additional concern for children even when active smoking is absent at home, or school environments remain contaminated from prior use31.
Health consequences are significant: beyond respiratory illness and asthma aggravation, well-documented globally recent research links adolescent SHS exposure to depressive symptoms32, negative emotions such as loneliness or anxiety, sleep disturbances, myopia progression, metabolic syndrome risk factors including dyslipidemia or insulin resistance, elevated blood pressure or hypertension risk, and under-five mortality in Sub-Saharan Africa24, academic performance deficits, increased susceptibility to future tobacco use initiation, even among never smokers, and clustering with other risky behaviors such as alcohol or drug use or e-cigarette experimentation.
Measurement approaches vary. While most studies rely on self-report surveys like GYTS/GSHS for cross-national comparability, despite recall bias concerns23, biomarker-based assessments using serum cotinine provide objective confirmation but remain less feasible for large-scale surveillance6. Future studies are needed to further understand determinants of adolescent secondhand smoke exposure2.
Limitations
This study has several limitations that should be considered when interpreting the findings. First, the cross-sectional design of the Global Youth Tobacco Survey limits the ability to establish causal relationships between SHS exposure and associated factors. The observed associations therefore reflect correlations rather than cause-and-effect relationships. Second, the study relied on self-reported data, which may be subject to recall bias, social desirability bias, and misclassification of exposure and behavioral variables. Adolescents may underreport or overreport tobacco exposure or related behaviors, potentially affecting the accuracy of the findings. Third, although multiple variables were adjusted for in the multivariable analysis, residual confounding may remain due to unmeasured factors such as household smoking rules, parental education, or neighborhood characteristics33.
In addition, the study included only school-going adolescents and therefore may not fully represent adolescents who are not attending school, who may have different exposure patterns. However, the Global Youth Tobacco Survey uses nationally representative sampling of school-going adolescents, which supports generalizability of the findings to this population in Zambia8,34. These limitations should be considered when interpreting the results.
CONCLUSIONS
Exposure to SHS among adolescents in Zambia remains high and is associated primarily with household smoking, peer influence, and smoking observed within school environments. Media exposure and tobacco-related behaviors were also associated with increased exposure, while demographic characteristics showed limited influence. These findings suggest that adolescents in Zambia are exposed to SHS across multiple social and environmental contexts. Continued monitoring of adolescent SHS exposure remains important. Further research may help clarify contextual drivers and long-term implications.